 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
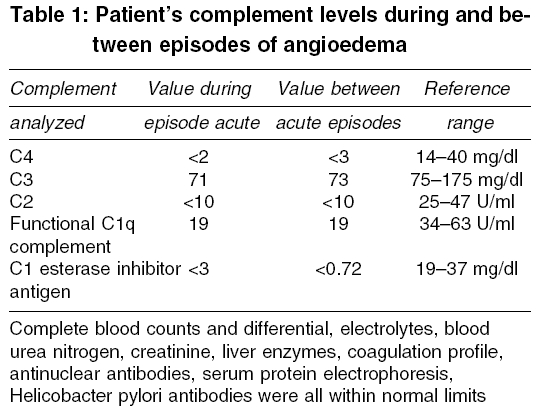
Indian Journal of Medical Sciences, Vol. 59, No. 10, October, 2005, pp. 451-454 Case Reports Acquired angioedema secondary to hormone replacement therapy Malani KumarA, Gupta C1 Departments of Pathology1, Heartland Regional
Medical Center, 5325 Faraon Street, St. Joseph, MO 64506, USA Code Number: ms05068 Abstract Angioedema is a potentially life threatening condition and may be either inherited or acquired. The latter is rare with only a handful of cases reported in the world literature. Presenting complaints are often vague. Those most commonly described include swelling in the subcutaneous and submucosal tissues. Patients presenting with laryngeal edema have high mortality, and high clinical suspicion is necessary to avoid instrumentation, which can precipitate laryngeal spasm. We present a review of reported cases of hormonally induced hereditary angioedema, along with a report of a patient with acquired angioedema secondary to hormone replacement therapy. To the best of our knowledge, this case probably represents the first reported case of acquired angioedema secondary to hormone replacement therapy.Keywords: angioedema; C1 esterase deficiency; serum protease; complement pathway C1 esterase is a protease that is normally inactivated by an inhibitor in the plasma, aptly called C1 esterase inhibitor (C1-INH). Deficiency of C1-INH leads to recurrent episodes of potentially life threatening subcutaneous and submucosal edema. This disease is termed angioedema and can be inherited or acquired, the latter very rare. We present a patient with an acquired deficiency of C1-INH while on hormone replacement therapy (HRT) along with a review of literature. Case report A 50-year-old lady presented with a soft tissue swelling of the jaw that started initially on the left side and appeared on the other side the following day. Review of her history revealed that she had sought medical attention for vague abdominal pains about a month earlier. A moderate amount of ascitis was reported on a computed tomography (CT) scan and ultrasound of abdomen. She had been experiencing severe episodes of abdominal cramps, vomiting, and occasionally diarrhea for the past 10 years. These episodes would occur 2-3 times per year but had increased in frequency more recently to every 4-6 weeks. They would usually last for up to three days. She denied any urticarial rashes. She was placed on HRT several years ago. In the past she had been extensively evaluated for abdominal symptoms, including coronary angiogram and colonoscopies, which were all normal. A physical examination was otherwise unremarkable. Suspecting C1-INH deficiency, a complement study was ordered. Blood samples were taken both during and between acute episodes and were sent for analysis to Mayo Clinic, USA [Table - 1]. Testing for complement deficiency in family members did not reveal any abnormality. A diagnosis of acquired C1 esterase deficiency was thus made. HRT was discontinued and therapy was initiated with 6mg/day of stanozolol as she did not tolerate initial treatment with danazol. Interestingly, the severity of abdominal pain decreased and she no longer had associated symptoms such as nausea, vomiting and diarrhea. Discussion Recurrent angioedema is a distressing and even life threatening condition and may be inherited or acquired.[1]-[2] Clinical symptoms includes episodes of swelling of face, extremities, and genitals, recurrent abdominal pains, occasional anorexia, nausea, vomiting, and ascitis. This latter condition may sometimes mimic acute abdomen and may lead to unnecessary surgical intervention. Undiagnosed gastrointestinal angioedema have occasionally been attributed to psychosomatization disorders, with unnecessary psychiatric referral. Edema of larynx, lips, tongue, and soft palate, and rarely asphyxiation due to laryngeal edema can occur with mortality reported to be as high as 30-40% due to upper airway obstruction.[3] Attacks are usually self limiting, generally lasting for 1-5 days and are followed by disease free interval of variable duration. Hereditary angioedema (HAE), which includes type I and type II, are related to C1 inhibitor (C1-INH) deficiency and are caused by mutations in the C1-INH gene.[2] The defective gene produces either no or low C1-INH (type I) or a dysfunctional C1-INH (type II).[2] Acquired angioedema (AAE) results from increased destruction or metabolism of C1-INH and is subdivided into types I and II. Type I AAE is associated with various disorders such as leukemias (chronic lymphocytic leukemia), lymphomas, various autoimmune and rheumatologic disorders, and some cancers.[2],[4],[5] These patients have circulating anti-idiotype antibodies against specific immunoglobulins expressed on the surface of B-cells. Immune complexes continuously activate complement component C1, thus C1-INH levels decrease, as synthesis cannot keep pace with consumption. In type II AAE autoantibodies (typically IgG but sometimes IgA or IgM) against C1-INH molecules are produced, bind at the active site of C1-INH molecule, leading to its inactivation. [10],[11] Other forms of angioedema occur include those secondary to angiotensinogen converting enzymes inhibitors (ACE-I), angiotensin receptor blockers (ARB), and urticaria associated angioedema.[1]-[2] Patients with AAE have significantly decreased serum levels of classical complement (C) components, C4, C2, and particularly C1q. Decreased serum C1q levels in AAE help distinguish it from HAE, in which C1q levels are usually normal. Angioedema from ACE inhibitor use can be distinguished from HAE and AAE only by history, C1-INH levels and complement assays. C1-INH has inhibitory effects on C1s and C1r and it also blocks the activity of other plasma proteases including kallikrein and factor XIIa that participates in bradykinin formation. The large amount of bradykinin released during acute attack of HAE or AEE due to subnormal C1-INH activity is thought to be responsible for most symptoms by directly causing increased vascular permeability (edema, swelling and ascitis), vasodilation (congestion, erythema and hypotension) and contraction of non-vascular smooth muscle (cramps, spasms and pain).[2] There are few case reports that hormone administration can lead to occurrence or worsening of angioedema episodes in women with HAE.[7],[8] Burke, et al in their large study of 516 women with angioedema found 46 patients with HAE who developed recurrent symptoms either upon initiating oral contraceptive use, or had exacerbation of their symptoms after starting oral contraceptives. They described 3 women with C1-INH deficiency whose angioedema was exacerbated by hormone replacement therapy.[8] A few other similar cases are described in the literature and were reviewed in the above paper. In contrast to these cases, our patient had no family history of angioedema and complement levels were normal in all family members tested. However, patient had low C1-INH and C1q levels, compatible with AAE. Her symptoms improved upon withdrawal of HRT and initiation of therapy with androgen analogues. It is hypothesized that estrogens affect the synthesis and degradation of bradykinin, precipitating symptoms in patients with HAE.[8] Also low plasma C1-INH levels are reported in women on oral contraceptives.[9] Estrogens lead to increased levels of factor XII and plasma prekallikrein.[8],[9] Other factors such as genetic polymorphism in the kinin system may play a role. Instrumentation of oropharynx is relatively contraindicated because of risk of inducing life threatening laryngeal edema. The treatment of choice for HAE is intravenous purified (vapour-heated) C1 esterase inhibitor concentrate.[10] If unavailable then androgen should be started immediately. Intubation and ventilatory support may be required. Nebulised recemic epinephrine and subcutaneous epinephrine early in an acute attack may prove life-saving.[2] Treatment of the underlying disease and methylprednisone may be helpful in AAE.[4] Attenuated androgens such as danazol and stanozolol can prevent symptomatic attacks in patients with HAE, and also selected patients with type I AAE.[11] Fresh frozen plasma (FFP) contains C1-INH and may abort episodes of acute HAE. Plasmin inhibitors such as tranexamic acid and E-aminocaproic acid may also be used for prophylaxis. Prophylactic administration of FFP, C1-INH concentrate, and attenuated androgens before any major surgical and dental procedure is necessary to prevent an acute attack of HAE. ACE inhibitors are contraindicated and estrogens should also be avoided. References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05068t1.jpg] |
| |||||||||

{kind=link}