 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 59, No. 10, October, 2005, pp. 455-456 Letter To Editor Parasites (filaria & strongyloides) in malignant pleural effussion Patil PrashantL, Salkar HarshaR, Ghodeswar ShekharS, Gawande JayantP Department of Medicine, Government Medical College,
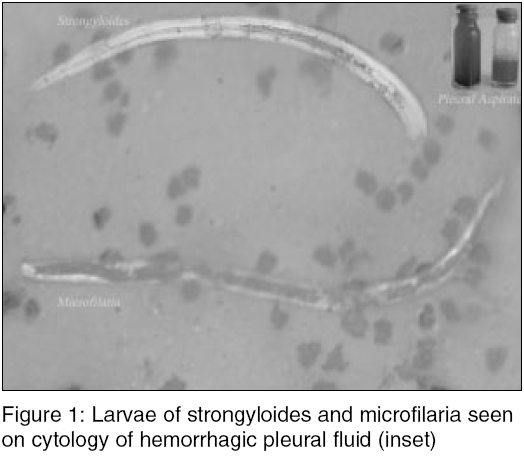
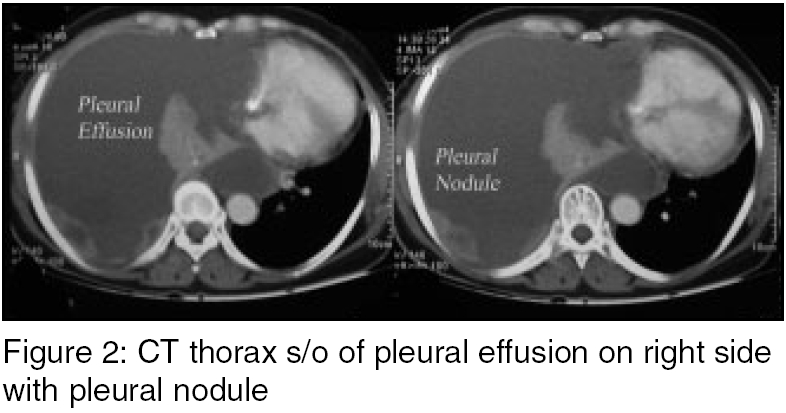
Nagpur, India Code Number: ms05069 Sir, Infections and malignancy are common causes of pleural effusion diagnosed by X-ray chest, ultrasound, CT thorax, and diagnostic paracentesis. Search for primary malignancy and rare infections may require special cytological examination and investigations. Multiple parasitic associations in malignant effusion have rarely been reported. A 48-year-old female, farm laborer presented with right-sided pleuritic chest pain, progressively increasing Dyspnoea, and nocturnal cough since 1 month. There was no significant history in past or family. She had respiratory rate of 30/min, pallor and right-sided pleural effusion, rest of the examination was normal. Investigations were: Hb - 9.0 g%, TLC - 9000/mm3, P - 60%, L - 32%, E - 8%. Absolute eosinophil count - 720. No hemo-parasites on peripheral smear. Tapping of right-sided pleural effusion, noted on chest X-ray, revealed exudative hemorrhagic fluid with 40% eosinophils, atypical malignant cells, and larvae of strongyloides and microfilaria [Figure - 1]. CT thorax was s/o of right pleural effusion with pleural nodule [Figure - 2], showing malignant deposits of adenocarcinoma on FNAC. Enzyme-linked immunosorbent assay (ELISA) for HIV I and II was negative. Albendazol and diethylcarbazine therapy showed clearance of the parasites from the pleural fluid in 1 week. The patient refused further investigation and went home with symptomatic improvement after therapeutic paracentesis. International travel to tropical countries has posed the travelers to risks and spread of diseases despite of quarantine.[1] Helminthic infestations elicit eosinophilia though definite evidence of pleuro-pulmonary involvement needs demonstration of ova or larva in the sputum, broncho-alveolar lavage, pleural fluid or lung tissue, or serology including ELISA and monoclonal antibodies.[2] The mechanisms by which helminthic parasites may cause pulmonary disease are:
Stongyloidiasis is characterized by watery diarrhea, abdominal cramping, and urticarial rash. Treatment includes ivermectin 200 mgkg/day for 2 days and/or thiabendazole 50 mg/kg/day in two doses for 2 days. A review describes the clinical manifestations, various diagnostic tests and treatment strategies.[3] Filariasis acutely presents with fever, adenolymphangitis, funiculitis, epididymitis, or orchitis. Lymphoedema, hydrocele, elephantiasis, chyluria are features of chronic filariasis. Diagnosis of filariasis is made by demonstrating microfilariae in the blood samples and body fluids.[4] Pleural effusion as a manifestation of filariasis has been reported rarely.[5] Treatment with diethylcarbamazine clears the effusion. Pleural effusion could be exudative or transudative. Malignancy is the commonest cause of hemorrhagic effusion seen with malignancy of lung, breast, and lymphoma or as adenocarcinoma from occult primary. The main presenting symptoms are Dyspnoea, cough, and chest pain. Ultrasound or CT guided thoracocentesis with cytological examination of the fluid aspirated or pleural biopsy improves the cytological yield to 80-90%. Thoracocentesis relieves symptoms and sclerotherapy gives 70-95% response rates References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05069f2.jpg] [ms05069f1.jpg] |
| |||||||||

{kind=link}
{kind=link}