 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 59, No. 11, November, 2005, pp. 471-479 Original Article Tilt-table testing as a predictor of + GZ tolerance Zawadzka-Bartczak E, Kopka L Department of Internal Disease, Polish Air Force Institute of Aviation Medicine, Warsaw Code Number: ms05072 Abstract BACKGROUND: G-tolerance assessment is an essential element of both military pilot and pilot candidate evaluation.AIMS: Attempt at prediction of individual relaxed + Gz tolerance on the basis of head-up tilt (HUT) testing. SETTINGS AND DESIGN: In two stages, 20 healthy men at the mean age 21.5 years took part in this study. The first stage, a 45 min, HUT test was performed using the Westminster protocol. During the second stage each underwent a centrifuge evaluation in response to gradual onset rate profiles. METHODS AND MATERIAL: In each subject, heart rate (HR) and blood pressure (BP) before and at 2, 15 and 45 min of the tilt-test were recorded. The gravity-load centrifuge (GOR) studies were carried out [following the standard GOR programme, at 0.1 G/s rate of gravity load increase until the gravity load tolerance limit (loss of peripheral vision) was reached]. STATISTICAL ANALYSIS USED: Relationships between variables were explored using Kendall's tau-B correlation coefficient. The critical P-level was one-tailed 0.05. RESULTS: In four of 20 subjects (20%), vasovagal syncope occurred during the tilt test. G-level tolerance of this group (of +Gz accelerations) lay in the range from +4 to +8.1 Gz, (+5.72 ? 0.86 Gz average) and was comparable to the group without syncope. Loss of consciousness did not occur in any subjects during the centrifuge test. No statistically significant correlation was observed between HR and BP during tilt test and tolerance to +Gz accelerations. CONCLUSIONS: The result of tilt testing, carried out according to the Westminster protocol, was not useful in predicting individual tolerance to +Gz gravity loads. Keywords: blood pressure; centrifuge examinations; vasovagal syncope Examination of cardiovascular responses to a programme of linearly increasing acceleration on a gravity-load centrifuge (GOR) is a routine test in the assessment of head-foot gravity load tolerance.[1] Since this programme uses a low rate of gravity load increase (0.1 G/s), actual efficiency of body compensatory mechanisms can be assessed in this programme. Regulation of changes of heart rate (HR) and blood pressure (BP) during the test depends on many factors, but one main element of adequate circulatory system adaptation to hydrostatic changes depends on normal function of high-pressure baroreceptors of the cardiovascular system. [2],[3],[4]The specificity of flying military aircraft, particularly highly-manoeuverable planes, is connected with effects of high +Gz gravity loads on pilot′s physiological performance. Pilot candidates must therefore meet not only clinical health criteria but also correctly react to gravity load-induced blood redistribution in the vascular bed. The +Gz gravity load shifts a significant volume of circulating blood to the lower parts of the body that is thought to provoke relative central hypovolemia.[3] This reduces venous return, cardiac output and stroke volume and decreases arterial pressure. In case of failure of compensatory mechanisms, this sequence leads to critical reduction of cerebral perfusion and loss of consciousness (G-LOC).[3] The response of the circulatory system to increasing gravity load includes increased activation of the sympathetic system followed by humoral activation. As a result of increasing sympathetic activation, peripheral resistance increases, HR accelerates, myocardial contractility increases and constriction of large veins and venous pooling in the viscera occurs. Furthermore, humoral activation (catecholamines, renin-angiotensin-aldosterone system and atrial natriuretic peptide)[5],[6] supports the defence mechanisms activated as a result of unloading of carotid-cardiac baroreceptors. The same mechanisms (blood redistribution and reflex response) occurs with body position change from recumbent to erect.[7] Baroreceptor function disturbances are responsible for orthostatic hypotension (vasovagal reflex and syncope) even in clinically healthy individuals.[8] It can be claimed, therefore, that one effect of +Gz gravity loading, with respect to the cardiovascular system′s reaction, is an exaggerated case of orthostatic stress. In clinical practice, head-up tilt (HUT) is the basic diagnostic test applied to otherwise, healthy, individuals who present clinically with recurrent consciousness disturbances. Its main purpose is to provoke symptoms of vasovagal syncope in a peripheral model of vasovagal reaction.[9] Thus, to test a GOR programme, HUT could be useful to assess (under monitored conditions) reflex reactions to hydrostatic changes. It seems that the underlying mechanisms may involve similar responses (syncope resulting from orthostatic stress and G-LOC) to both tests. In this respect, HUT has potential to be a first screening test for candidate acceptance. In view of the fact that the cost of gravity load testing is very high, and determination of tolerance to acceleration is an indispensable condition to qualify a candidate for aviation training, new, less expensive methods to carry out this assessment could be beneficial. The aim of the study was to attempt at prediction of individual relaxed + Gz tolerance on the basis of HUT testing. Materials and methods The study group included young, clinically healthy (without history of syncope) males (volunteers) aged 20-30 years (mean age 21.5 years), weighing 65-80 kg and of 165-180 cm height who were normotensive, nonsmokers and not on medication. Each gave written consent to participate in the study. An ethics committee of the Polish Air Forces Institute of Aviation Medicine cleared the protocol for execution of the study. Study 1: HUT SBP, diastolic blood pressure (DBP), mean arterial pressure (MAP) and HR before and in 2, 15 and 45 min of tilt test were evaluated. Study 2: centrifugation
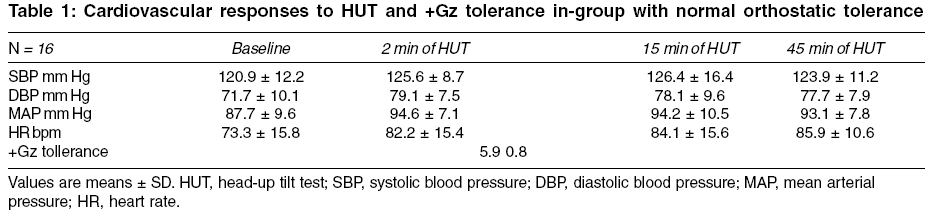
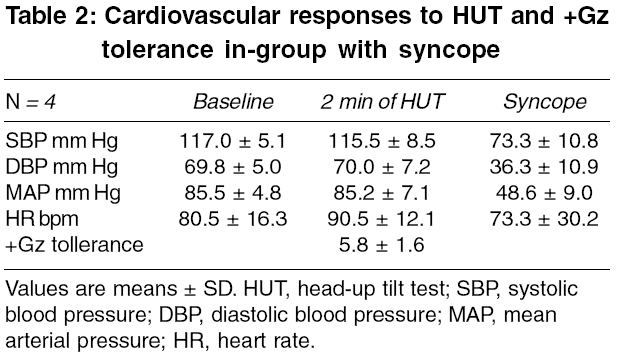
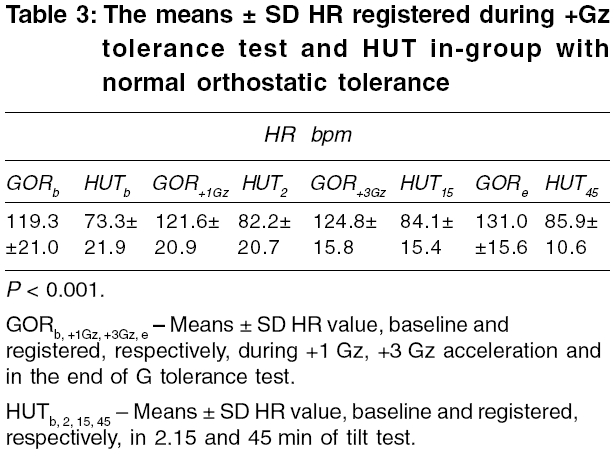
The tests were performed in the morning between 9 a.m. and 11 a.m., after a light breakfast and night of normal sleep. During the test, the subject remained in the seated position in the centrifuge gondola. Constant radio contact was maintained between the subject and the doctor conducting the test. During the test duration, the subject′s behaviour was monitored on a TV-screen at the control desk. During the test, we measured the reaction time to light stimuli - lamps switched according to program and placed symmetrically in the peripheral field of vision at 180° angle. The subject confirmed the received light stimuli by pressing a button on the lever with their fingers. Throughout the +Gz examination only ECG (HR) was continuously recorded to monitor possible heart rhythm disturbances. BP was not monitored during the +Gz tolerance tests due to difficulty with maintaining signal integrity and the limited value of baroreflex measures in predicting maximal +Gz tolerance.[4] The subjects were instructed to remain as relaxed as possible (to ride without muscular contraction and anti-G straining maneuvers were not performed) and did not wear a g-suit. A GOR was defined as ′successful passing′ at +5.5 Gz level. A result below that, indicated poor tolerance of acceleration and disqualified a potential candidate from aviation training. In each subject HR and BP, recorded before and at 2, 15 and 45 min of the tilt test (or at the time of syncope occurrence), were correlated with their G-tolerance level. The mean HR response between the HUT (at 2, 15 and 45 min) and GOR (at +1 and +3Gz and threshold of tolerance) were correlated. Because of small groups, the relationships between the data were explored using Kendall′s tau-B correlation coefficient. The critical P -level was one-tailed 0.05. Results In four of 20 subjects (20%), vasovagal syncope occurred during the tilt test. In all cases this was a vasodepressive reaction that developed between minutes 15 and 17th (16.2 ± 0.9 min average). In the remaining males, a normal orthostatic reaction occurred. None of the four syncopal subjects had visual symptoms prior to HUT-induced symptoms. G-level tolerance of this group (of +Gz accelerations) lay in the range from +4 to +8.1 Gz, (+5.72 ± 0.86 Gz average). Loss of consciousness did not occur in any subjects during the centrifuge increase in gravity load. During centrifuge tolerance testing, two individuals with vasovagal syncope demonstrated poor acceleration tolerance (+4 and +5.2 Gz) while two other syncopal subjects tolerated acceleration well and very well (+6.2 and +7.9 Gz). The fact is worth stressing that in as many as five individuals (25%) in whom vasovagal symptoms failed to develop, tolerance to acceleration was very poor (below +5.5 Gz) and, in one, even poorer than subjects with syncope during the tilt test. Cardiovascular responses to HUT and +Gz tolerance in the group with normal orthostatic tolerance and the group with syncope are presented in [Table - 1] [Table - 2], respectively. There were no statistically significant differences in the SBP, DBP, MAP and HR baseline and 2 min of HUT in both groups. In the group with abnormal orthostatic reaction, the onset of the fall in BP was unpredictable. Once begun however, it progressed rapidly with sustained decreases in SBP, DBP and MAP. The means SD of HR, registered during +Gz tolerance test and HUT in the group with normal orthostatic tolerance, are presented in [Table - 3]. There were statistically significant differences ( P < 0.001) between HR registered during +Gz tolerance test and HUT in selected periods of measurements. No statistically significant correlation was observed between SBP, DBP and MAP and HR registered before and in 2, 15 and 45 min during tilt test and tolerance to +Gz accelerations. Discussion In the present study the relationship between cardiovascular reflexes during passive HUT and +Gz tolerance test was assessed. Is tolerance to true orthostasis and simulated orthostatic stimulus (head-to-foot acceleration at higher than +1 Gz level) the similar thing? The results of the current study suggest that although HUT and +Gz acceleration test involves cardiac baroreflex response in the same mechanism (of redistribution of blood from head-to-foot), the individual cardiovascular reactions to both tests may be differ. Vasovagal reaction is the most frequent cause of syncope in cases diagnosed to be of unclear origin (about 40%). That type of fainting occurs often even in young, clinically healthy individuals. In the Framingham study, at least one syncopal episode during a 2-year follow-up was found in 3% of males and 3.5% of females.[11] In a study involving 3000 US Air Force personnel members (mean age 29.1 years), at least one syncopal episode (occurred spontaneously) was observed in 82 individuals (2.7%).[12] In our study, a, positive tilt test was obtained in 20% of males and none of them experienced previous syncopal episodes. Loss of consciousness caused by gravity load (G-LOC) during real combat sorties poses a threat to pilots′ lives. Therefore, during aviation training, cadets are taught to ′counteract gravity loads′ by means of special practices. Manoeuvres causing tension of appropriate groups of muscles combined with a special respiratory technique (modified Valsalva manoeuvre), have been shown to increase acceleration tolerance by as much as +2 G.[13] Results from that study demonstrated however, that these manoeuvres exerted no effect on baroreflex activity. Individual tolerance to +Gz gravity loads depends mainly on normal (reflex) reactions of the circulatory system. Thus, it may be presumed that if vasovagal reaction to tilt stimulus provides evidence of an abnormal reflex, then tolerance to +Gz gravity loads would be poorer. This was not confirmed by results of the present study. The mean tolerance to +Gz gravity loads in individuals in who vasovagal syncope was provoked was comparable with that obtained in the remaining study subjects (+5.82 vs +5.94). Therefore, it is interesting that a stimulus of a similar type but significantly stronger, i.e. +Gz gravity load, caused no syncope, even in individuals with abnormal orthostatic reaction to HUT. It is commonly known that the gravitational force creates pressure gradients in the circulation. For tilting and centrifugation, local arterial pressure change from gravitational stimulation is calculated as pressure (P) at a distance h from the arterial hydrostatic indifference level, applied along the z (head to foot) body axis according to the following expressions: P = pg [sinθ] - for tilt and P = ph (ω2/ rh) -for centrifugation.[1] In accordance with this reasoning the brain level BP during HUT should be higher then during GOR. It has been demonstrated[14] that exposure to hypergravity influences cerebral autoregulation in humans. The particular finding that dynamic autoregulation was impaired in the supine position but restored in the upright position after intraocular pressure at was lowered specifically suggests that exposure to hypergravity results in a leftward shift of the static cerebral autoregulation curve. Although, the mechanism for this proposed shift is unclear, it may involve adaptation to reduced cerebral perfusion pressure during +GZ exposure and/or possibly a vestibular-mediated effect on nervous pathways that modulate cerebrovascular tone. Similar studies have been published attempting to correlate physiological responses to lower body negative pressure (LBNP) with G-tolerance; these failed too.[15],[16] In those studies, differences in calf, thigh and abdominal segment blood volume changes, and carotid-cardiac baroreflex sensivity confirmed that LBNP effects were not sufficiently similar in nature to the acceleration environment. Lack of correlation between tilt and gravity load tolerance tests may also be as a result of different hormonal responses to the two stressors. During centrifuge tests, serum adrenaline, noradrenaline, renin, aldosterone and vasopressin concentrations have been shown to increase significantly while atrial natriuretic peptide and cortisol levels decrease.[5],[17] However, during those centrifuge tests, increases in hormone concentrations were observed throughout the whole test period and for about 2 min after test completion, while in HUT it depended upon the phase of the test. This was confirmed by results of our study. Mean HR was significantly higher during GOR than during HUT. During GOR, HR increased systematically together with +Gz accelerations. During HUT, HR increased only in the first 2 min and after 15 min of the test. It has been demonstrated in numerous studies that, during tilting to erect position or HUT, noradrenaline, adrenaline and vasopressin concentrations increased significantly after several minutes of the test, reaching a constant value, which remained unchanged until test completion. [18],[19],[20] This was true, even if a significant BP decrease and/or HR reduction (fainting) developed in the subject.In addition, the Renin-Angiotensin-Aldosterone (R-A-A) system activation occurred only after about 15-20 min of HUT.[20] In our HUT study, syncope developed between minutes 15th and 17th. It was highly probable that it was a disturbance in R-A-A system activation that was responsible for this event, especially since, after 20 min of the test, systolic and diastolic pressures increased in relation to baseline values in as many as 9 and 12 remaining individuals, The fact is worth stressing that the centrifuge test was accompanied by significantly greater emotional stress, responsible for increased adrenaline secretion, which may be a condition of good tolerance of gravity loads and may prevent loss of consciousness even in individuals with vasovagal reaction during HUT. It should however, be mentioned that although tests on the centrifuge were always conducted according to the same programme, tilt test protocols, during which hormonal concentrations were assessed, varied significantly from ours and from each other. Undoubtedly, different tilt angles of the table and divergences concerning test duration affected the type and degree of hormonal response.[19] Besides, for reasons not elucidated as yet, tilt test results could be false positive.[21] It is also possible that different mechanisms may be associated with different reactions of the cardiovascular system during orthostasis and +Gz acceleration tests. It is commonly known that linear accelerations and gravity are perceived by the otolith organs of the vestibular apparatus.[22] It was previously demonstrated[23] that bilateral transection of the vestibular nerves in paralyzed, anaesthetized cats impaired reflex compensation for orthostatic hypotension produced by HUT. This finding suggested that the vestibular system was involved in BP regulation during postural changes. However, to our knowledge, there have not been many studies showing possible influences of the otolith system on the cardiovascular system in humans during HUT test and head to foot accelerations. It has been demonstrated that the interaction of the baroreflexes and the vestibulosympathetic reflex (VSR) is additive during LBNP and head-down rotation.[22] Yates and co-workers have reported that the baroreceptor and vestibular reflex pathways (in cats) remain separate until they synapse on the presympathetic neurons in the rostral ventrolateral medulla.[24],[25] However, electrical stimulation of the vestibular nerve has been demonstrated to activate a few neurons in the nucleus tractus solitarii, which is the first central synapse of the baroreflex.[26] Although, these two cardiovascular reflexes do not appear to interact centrally to modify sympathetic outflow during an orthostatic challenge, they certainly complement each other. It might be speculated that, during movement or a change in posture, the VSR acts immediately to defend against a possible hypotensive episode before a drop in arterial pressure is sensed by the baroreceptors. Thus the VSR feed-forward property would aid in the stabilization of arterial pressure before the baroreflexes are engaged.[27] In summary, our results indicate that, although, the cardiovascular stimulus for activation of reflex mechanisms compensating gravitational redistribution of blood during centrifuge and tilt tests is similar, circulatory system reactions were different. This difference could be attributable to differences in barorereflex activation, involvement of vestibular inputs, hydrostatic gradient differences, activation timetables of hormones or other, as yet undetermined, physiological determinants of cardiovascular regulation. Conclusion The result of tilt testing, carried out according to the Westminster protocol, was not useful in predicting individual tolerance to +Gz gravity loads.References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05072t2.jpg] [ms05072t3.jpg] [ms05072t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}