 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 59, No. 11, November, 2005, pp. 488-494 Original Article Rapid assessment survey of earthquake affected Bhuj block of Kachchh District,* Gujarat, India Pawar AT, Shelke S, Kakrani VA Department of P. S. M., B. J. Medical College, Pune,
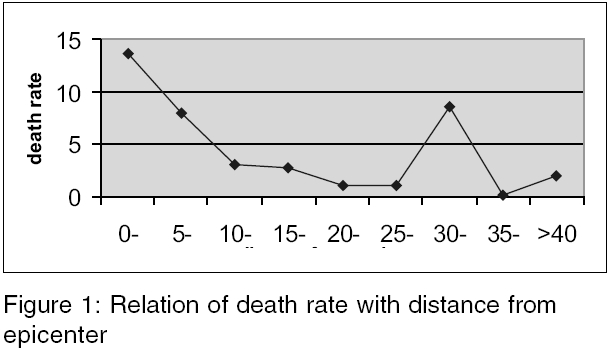
India Code Number: ms05074 Abstract RESEARCH QUESTIONS: How much human loss would have caused by the earthquake in Bhuj block? What is the environmental sanitation status?OBJECTIVES: (1) To assess human loss and injuries after the earthquake in Bhuj block.(2) To study the status of some relief activities.(3) To study the environmental sanitation status of the earthquake affected Bhuj block. STUDY DESIGN: Cross-sectional study. SETTINGS: Bhuj block. Participants: All villages excluding Bhuj city of Bhuj block. Statistical analysis: 0 Proportions, chi-square test, chi-square for trend. RESULTS: Survey was done in 144 villages; there were total 541 deaths with death rate of 3.18 per 1000 population. Death rate was significantly associated with distance of village from epicenter (chi-square for trend significant, P < 0.001). Among victims, majority were children 171 (45.4%) and women 107 (28.4%). Relief work was significantly associated with accessibility of village (P < 0.001) and few interior pockets were deprived of help. Total 56 (38.9%) villages were entirely dependent on water tanker for water supply and in 61 (42.4%) villages drinking water was used without chlorination. In 142 (98.6%) villages open-air defecation was practiced. Diseases such as URTIs, diarrheal diseases, fever and conjunctivitis were commonly observed in the field area. Keywords: Bhuj block; earthquake; rapid assessment On Friday, 26 January 2001, around 8.46 a.m., when Indian Republic Day celebration was underway, one of the most devastating natural calamities of our time ravaged the state of Gujarat. The earthquake of intensity 6.9 Richter scale flattened Bhuj city and badly struck Bhachau, Anjar, Rapar and Gandhidham blocks of Kachchh district and spread over radius of 200 km. Bhuj, once a historical town and vibrant market, became a death trap, neither the military station nor the air force camp escaped quakes fury. Hundreds of NGOs and thousands of volunteers from India and abroad traveled a great distance to help victims and assisted thousands of people in rebuilding their lives. Along with many deaths and severe injuries requiring medical intensive care increased risk of communicable diseases remains a potential risk following natural disasters. This is mainly due to overcrowding and deterioration in environmental hygiene particularly affecting water supply and disposal of human wastes. This again depends upon previous sanitary levels of area.[1] Diarrheal diseases are a major cause of mortality and morbidity in emergencies; hence continuous check on water supply and disposal of human wastes are of utmost importance.[2] The process of assessment is as essential in relief work as in developmental work, though in emergency we cannot wait to find out all available information before responding.[3] Rapid initial assessment to identify immediate problems in affected area should be done.[4] So rapid assessment survey of earthquake affected Bhuj block was done, to assess human loss and injuries after earthquake, to study environmental sanitation status of earthquake affected Bhuj block and status of some relief activities. Materials and methods A rapid assessment survey was done in Bhuj block of earthquake affected Kachchh district during a period of 6-10 February 2001. ′Kachchh Navnirman Abhiyan′ one of the nodal NGO involved in relief work provided all essential assistance throughout study. Survey was done by a group of 18 people (15 doctors and three paramedical workers from Pune), who were divided into five teams. Each team was provided one volunteer and one local guide, who were familiar with local language and locality by ′Kachchh Navnirman Abhiyan.′Each team carried a kit of essential medicine with them. Each team was allotted a defined geographic area. A map of Bhuj block compiled by CMAG-EPC earthquake technical assistance cell was given to each team. A proforma was prepared for recording data from each village regarding human and animal deaths and injuries, available water sources, chlorination of water, sanitation facilities, illness if any, necessities of villagers, status of relief activities, etc. A team approached each village and identified key informants such as local leaders (Sarpanch) and teachers. Data were collected by interviewing key informants as well as through group discussions. Data regarding environmental and water sanitation conditions were collected by exploratory walk. People with disease if any were examined and given medicines. Present study was planned in emergency at head office of ′Kachchh Navnirman Abhiyan′ one of the nodal NGO involved in relief work. Along with team members, representatives of ′Kachchh Navnirman Abhiyan′actively participated in planning present study. Social scientists of Tata Institute of Fundamental Research approved the study design. As present study does not consist any kind of intervention or procedure that ethically cannot be approved. Planning committee decided to go with study without any ethical approval. Also due time constraint and lack of facilities to approach any ethical committee considering emergency situation of earthquake; it was not practically feasible to approach any ethical body. Collected data were presented in tables and graphs and analyzed by using appropriate statistical tests. Data generated in the present study were qualitative data. To test the association between two qualitative variables chi-square test was used. To test the trend of death rate along with increasing distance from epicenter chi-square for trend was used. Results Total 144 villages, 128 from Bhuj block and 16 from adjacent blocks, were surveyed. We came across nine uninhabited villages during our survey. Population of these villages was approximately 170 000. Total deaths reported from these villages were 541, giving death rate about 3.18 per thousand population. Total 1412 injuries were reported from these 144 villages, while five persons were missing. There were 769 animal deaths. Out of total 541 deaths in area, age, and sex composition of 376 was available; [Table - 1] age and sex composition of 165 deaths from Sukhpar town was not available. Among deceased, majority of them, i.e., 171 (45.4%), were children below 14 years of age, while 28.4% were adult females and 10% were adult males. Thus, children and females comprised 81.6% of deceased. Relation of human loss against distance from epicenter shows attenuation tendency as distance from epicenter increases death rate goes on decreasing [Table - 2], [Figure - 1]. Death rate in villages, at a distance 30-35 km from epicenter, was exceptionally high, i.e., 8.52 per 1000 population. This was due to town Sukhpar, which was urban area with population of 10 000, with many multistory building and reported 165 deaths at death rate of 16.5 per 1000 population and hence death rate in this category was high. To assess status of relief activities, three parameters, i.e., restoration of electricity, help provided by NGOs and food distribution from public distribution system (ration) were considered [Table - 3] [Table - 4]. Villages with kachha (mud) approach road were considered as hard to reach interior pockets. It was observed that relief activities in interior villages were inadequate. Of the total 144 villages surveyed 90 (62.5%) villages had pucca (tar) approach road, while 54 (37.5%) were having kachha (mud) approach road. In 28 (51.8%) villages with kachha approach road, electricity was not restored. While, in only 16 (17.8%) villages with pucca (tar) approach road electricity was not restored. This difference is statistically significant ( P < 0.001). Among villages with kaccha (mud) approach road nine villages received inadequate help from NGOs, while two villages received no help at all. In this study, adequate help was defined as supply of one tarpaulin per family, two blankets per family and food materials for 15 days for family. Ideally tent per family and blanket per person was required but there was shortage of tent and blankets. State government of Gujarat was supplying food materials to earthquake victims through its public distribution system. About 15 (68%) villages with kachha road had not received food from public distribution system till the time of survey. All these relief activities were significantly associated with condition of approach road to village ( P < 0.001). Of these 144 villages 21 (14.6%) villages were depending entirely on local sources such as well, tube-well, and lake for water. In 51 (35.4%) villages, water was provided by pipeline of these 13 (9.0%) villages were having local sources of water in addition to pipeline [Figure - 2]. In 22 (15.3%) villages water-carrying pipeline was damaged due to quake and now these villages have to depend on water tanker for water. Of these 144 villages only 65 (45.1%) villages were receiving adequate water so as to take daily bath. Separate pipelines for high caste and low caste people were unique picture observed in few villages. When asked about the chlorination it was revealed that in 61 (42.4%) villages chlorination was not practiced. Most of the organizations providing relief materials were distributing chlorine tablets but they were not insisting on the use of these tablets. While assessing environmental sanitation status of villages, it was observed that the practice of open-air defecation was almost universal in the area. In 109 villages, there was no concept of sanitary latrines. In 17 villages, sanitary latrines were provided by NGOs prior to quake but 90% of them were damaged in quake. In 142 (98.6 %) villages, majority of people were practicing open-air defecation. In most of temporary settlement camps, there was no provision of sanitary latrines and people have to go for open-air defecation. Authors were like to throw light on very alarming and surprising fact that most of the volunteers and even doctors working in the area had no other option than open-air defecation. This can be attributed to the fact that most of the teams of doctors, who visited the area, were without public-health experts and sanitarians. Fortunately due to scarcity of water in Kachchh region of Gujarat, there was no breeding of mosquitoes. During survey 169 cases of upper respiratory tract infections, 36 of diarrheal diseases, 57 cases of fever, and 46 of conjunctivitis were identified and treated [Figure - 3]. Discussion In the morning of 26 January 2001 an earthquake of intensity 6.9 Richter scale, with epicenter 20 km northeast of Bhuj hited the western state of Gujarat. Total 7906 villages from 182 blocks from 21 districts were affected taking death toll of 20 005.[5],[6] Kachchh district alone reported 18 416 deaths, which was almost 92% of total human loss.[5] In the present study, 541 deaths were reported from 144 villages giving death rate of 3.18 per 1000 population. According to Japanese agency, death rate in Kachchh district was 12.1 per 1000 people. Bhachau taluka suffered highest ratio of human loss amounting to 6.47%.[7] Fewer death rates were observed in our study this can be attributed to fact that, majority of deaths were in Bhuj city and we surveyed rural area. In rural area people had left for their work in field in early morning and many people were attending Republic day celebrations in schools. UNDP reports similar finding. According to this report, in Kachchh district, 69% of human loss occurred in urban area and 31% in rural area. The cause of more fatalities in urban areas can be explained by multistory dwellings and apartments destroyed in urban area and streets filled with enormous amount of debris which made search and rescue more difficult.[8] Children and females comprised 81.6% of deceased. Among deceased 45.4% were children and 36.2% were females thus together they formed 81.6% of deceased. According to 1991 census, in total, they comprise (64.4%) of population.[9] The quake struck at 8.46 in the morning, when women have engaged themselves in ′care sector′ activities such as preparing meals, washing clothes and house cleaning. Under five year olds were with them; therefore, there was incidence of more fatalities among women relative to males. It means that during emergency this group is at more risk. There was inverse relationship between the distance of village from epicenter and death rate. The same observation has been reported by the Japanese agency.[7] It can be concluded from this observation that in early days of emergency village near epicenter need more attention. In the villages at a distance more than 45 km death rate observed was little high. These included mainly villages from Khavada area of Bhuj block. In this area due to cold people were at home in the early morning at the time of earthquake, also this region the houses were made of mud, which totally collapsed in earthquake. In the early days of emergency, there were many gaps and overlaps in providing relief work. Due to difficult roads, many hard to reach interior pockets were deprived of help while few villages on high ways received help in excess. Some of volunteers and NGOs were in so hurry of providing help that they really dumped the relief material in villages. URTI, diarrheal diseases, fever and conjunctivitis were commonly observed disease during survey. After earthquake, houses were either collapsed or damaged and people were living in temporary shelters. There was overcrowding hence there may be more cases of URTI and conjunctivitis especially in children. National disaster management cell of India had reported 32 cases of diarrhea, 49 cases of fever, and 71 of conjunctivitis in Bhuj on 14 March 2001 but no case of URTI has been reported.[10] The WHO reported that at the onset of disaster epidemic, a concern but no major epidemic had occurred, although, some expected cases of diarrheal diseases and acute respiratory tract infections had been noted.[11],[12] From this study, it can be concluded that rapid assessment survey is important tool in providing information for planning relief activities and rapid assessment survey should be done within first 2-3 days of emergency. From observations in study, it is recommended that there should be co-ordination between NGOs/agencies providing relief work and each NGO should shoulder specific responsibility in specific geographic region to avoid duplication of services and missing some interior pockets. Acknowledgment Authors express their sincere gratitude to authorities of Janpath citizen′s initiative and Kutch Navnirman Abhiyan or providing all essential help for present study. The co-operation extended by Dr. Prasad Rajhans (team leader), Secretary Emergency Medical Services, Pune, in study and preparing paper is also acknowledged. Thanks are also due to all our team members, NGO representatives for their participation in study.References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05074t4.jpg] [ms05074t1.jpg] [ms05074f1.jpg] [ms05074f3.jpg] [ms05074f2.jpg] [ms05074t2.jpg] [ms05074t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}