 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 59, No. 11, November, 2005, pp. 495-498 Case Reports Cesarean scar endometriosis - Report of two cases Goel P, Sood SS, Romilla1, Dalal A2 Departments of Obstetrics and Gynaecology,1Pathology
and 2Surgery, Government Medical College and Hospital, Chandigarh,
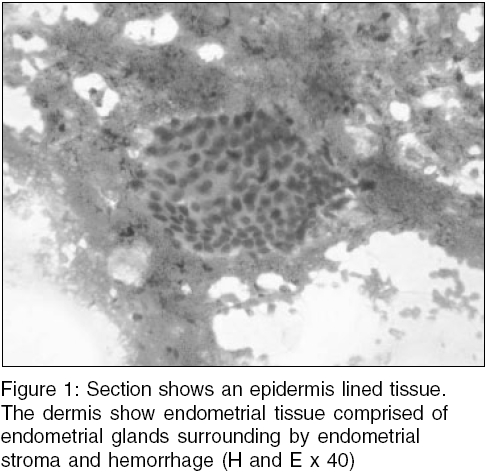
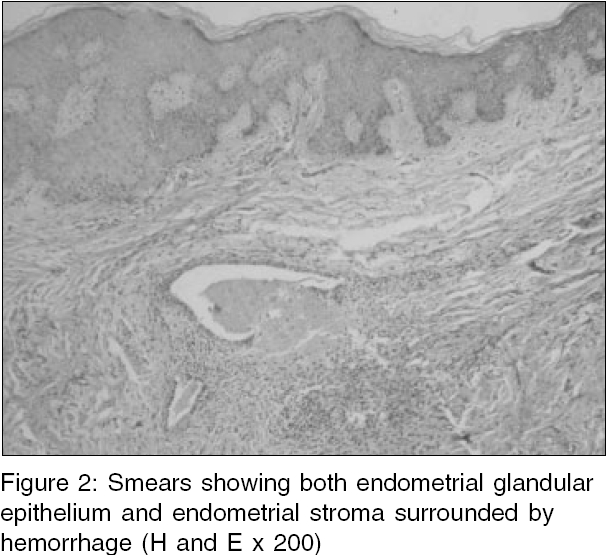
India Code Number: ms05075 Abstract Endometriosis is presence of functioning endometrial tissue outside the uterine cavity. Endometriosis can sometimes occur in a previous surgical scar. Scar endometriosis is rare and difficult to diagnose. It mostly follows obstetrical and gynecological surgeries. This condition is often confused with other surgical conditions. We are reporting two cases of scar endometriosis following cesarean section, which were misdiagnosed as stitch granuloma initially. Medical treatment was not helpful. Both the patients required wide surgical excision of the lesion. The pathogenesis, diagnosis and treatment of this condition are being discussed.Keywords: abdominal wall; endometrioma; endometriosis; scar endometrioma External endometriosis is defined as the presence of uterine mucosa (glands and stroma) outside the uterus. The most common location is within the pelvis and has been reported to occur in as many as 44% of women undergoing laparoscopy for nongynecological symptoms.[1] However, extra pelvic endometriosis is a fairly uncommon disorder and difficult to diagnose. The various sites for extra pelvic endometriosis are bladder, kidney, bowel, omentum, lymph nodes, lungs, pleura, extremities, umblicus, hernial sacs, and abdominal wall.[2] Abdominal wall endometriomas often develop in previous surgical scars but there is a case report of a spontaneous occurrence also.[3] Majority of the scar endometriosis have been reported after obstetrical or gynecological procedures such as cesarean delivery, hysterotomy, hysterectomy, episiotomy, and tubal ligations, [4],[5],[6] but few case reports are following appendecectomy, in the laparoscopic trocar tract, amniocentesis needle tract. Scar endometriosis patients are often referred to the general surgeons because the clinical presentation suggests a surgical cause. In a study by Blanco et al[7] the diagnosis was initially confused with inguinal hernia, incisional hernia and abdominal wall tumor. We report two cases of scar endometriosis following cesarean section over a period of 8 years. These two cases first reported to general surgeons where they were misdiagnosed as stitch granuloma. This paper is meant to increase the awareness regarding this rare condition, which is often misdiagnosed. Case reports Case 1 Case 2 Discussion Endometrioma is a well-circumscribed mass of endometriosis. Abdominal wall endometriomas presents as a painful swelling resembling surgical lesions such as hernias, hematomas, granulomas, abscess and tumors. So that is why these cases first report to general surgeons. Our two cases also reported to general surgeons first where a diagnosis of stitch granuloma was made. Scar endometriosis most commonly occurs after operation on the uterus and tubes. Incidence of scar endometriosis following hysterotomy is 1.08-2% where as after cesarean section the incidence is 0.03-0.4%.[6] The reason for higher incidence after hystertomy has been given as the early decidua has more pleuripotential capabilities and can result in cellular replication producing endometriomas. Time interval between operation and presentation has varied from 3 months to 10 years in different series. The etiology of abdominal wall endometrioma is thought to be a result of transportation of endometrial tissue during surgical procedures and subsequently stimulated by estrogen to produce endometriomas. The simultaneous occurrence of pelvic endometriosis with scar endometriosis is infrequent.[6] Our patients also did not have associated pelvic endometriosis. Preoperative diagnosis is difficult to make and sometimes the diagnosis is made after excision only. We could make preoperative diagnosis in one patient with FNAC. Various diagnostic methods have been described in the literature. Till recently the use of ultrasonography (USG) have hardly been reported in detail and anecdotal reports have described it as nonspecific, can give a varied picture of hypo echoic mass with scattered internal echoes. Recently a large series of 12 patients where USG and color Doppler substantially contributed to the correct preoperative diagnosis[8] and authors suggest that sonographic and color Doppler when combined with clinical data may substantially contribute to the preoperative diagnosis. FNAC has been reported to be accurate in diagnosis but in a recent report by Dwivedi et al. FNAC was not diagnostic in any of the four patients who underwent this procedure.[9],[10] Anecdotal studies have mentioned the use of computed tomography (CT) and magnetic resonance imaging (MRI) in making a diagnosis. CT usually shows a solid, well-circumscribed mass. MRI can be more helpful when the lesion is small because of its high spatial resolution, furthermore it perform better than CT scan in detecting the planes between muscles and abdominal subcutaneous tissue.[11] Treatment of choice is wide excision of the lesion and may sometimes require mesh placement as was done in our two patients. Medical treatment with the use of progestogens, oral contraceptive pills, and danazol is not effective and gives only partial relief in symptoms. Recently there has been report of use of gonadotrophin agonist but only with the prompt improvement in symptoms with no change in the lesion size.[12] These patients need to be followed up because of the chances of recurrence, which require re-excision. In cases of continual recurrence possibility of malignancy should be kept in mind. To prevent the occurrence of scar endometriosis it has been suggested that at the end of surgery especially on uterus and tubes, the abdominal wall wound should be cleaned thoroughly and irrigated vigorously with high jet solution before closure.[13] To conclude, one should have high index of suspicion of scar endometriosis when a woman presents with a painful swelling in the abdominal scar especially with a history of previous gynecological or obstetrical surgery. This condition can be confused with other surgical conditions. Efforts should be made to make a preoperative diagnosis with the help of imaging techniques and FNAC. Medical treatment is not helpful. Wide excision is the treatment of choice. Patient should be followed-up for recurrence. References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05075f1.jpg] [ms05075f2.jpg] |
| |||||||||

{kind=link}
{kind=link}