 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 59, No. 11, November, 2005, pp. 499-502 Case Reports Sarcoma-like mural nodules in ovarian mucinous cystadenomas - A report of two cases Chakrabarti S, Konar A, Biswas S, Das S Department of Pathology, NRS Medical College and Midnapur
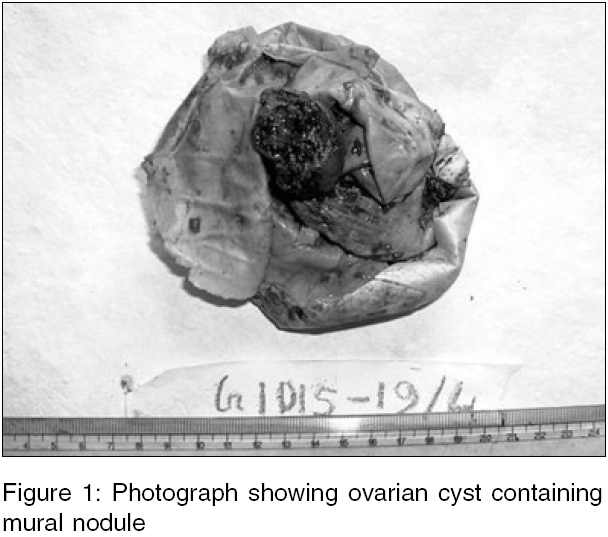
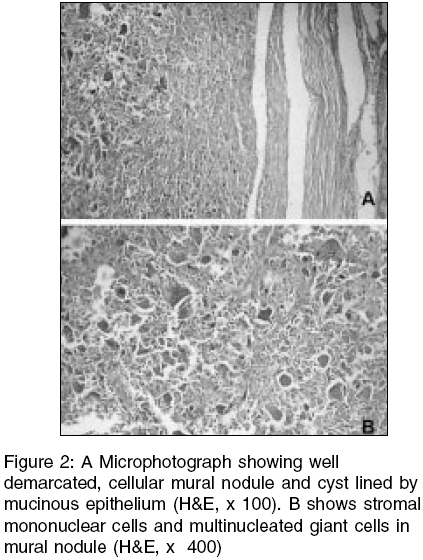
Medical College, Midnapur, Kolkata, India Code Number: ms05076 Abstract Sarcoma-like mural nodule is a very rare occurrence in a mucinous tumour of the ovary. Two such nodules having morphologically benign features with osteoclastic giant cells, in the wall of mucinous cystadenoma are described. In addition, these nodules exhibited reactive vascular proliferations. The sarcoma-like nodules are associated with a favourable outcome and must be distinguished from other malignant nodules composed of sarcoma or anaplastic carcinoma that may also occur in the wall of mucinous ovarian tumours.Keywords: mucinous tumour of the ovary; mural nodule; sarcoma-like nodule Ovarian mucinous tumours account for 15% of all ovarian neoplasms. Rarely, these cystic tumours may contain sarcoma-like mural nodules in their wall.[1],[2] Distinction of these lesions from true sarcomatous nodules and foci of anaplastic carcinoma is essential for the two latter tumours have a worse prognosis compared with the favourable behaviour of the sarcoma-like mural nodules.[2] Two cases of sarcoma-like mural nodules are described. Case reports Case 1 Grossly the ovarian cyst measured 12 x 11 cm. The outer surface was whitish and smooth. The cut surface showed multiloculation with clear mucinous fluid. An inner surface elevation (4 cm in diameter) was seen in one large locule [Figure - 1]. Cut surface of the nodule was homogeneous and brownish, resembling an old clot. Microscopically, the nodule was well demarcated, cellular, and contained stromal mononuclear cells and multinucleated osteoclast-like giant cells along with many dilated vascular channels and hemorrhagic areas. Cellular atypia and mitotic figures were absent. Other areas of the cyst revealed the characteristic histology of a mucinous cystadenoma [Figure - 2] without atypia, multilayering, or invasion. Case 2 Grossly, the right ovary was cystic and measured 22 x 18 cm. The outer surface was smooth and greyish-white. On section, a mural nodule was found inside the cyst wall, 4.5 cm in diameter and brown in colour. Microscopical examination of the cyst showed features of a mucinous cystadenoma. Sections from the nodule showed sheets of round to polygonal cells with variable amount of cytoplasm without nuclear atypia, osteoclastic giant cells, and inflammatory cells including histiocytes. Thus, in both cases, the diagnosis was mucinous cystadenoma with sarcoma-like mural nodule. Both patients are asymptomatic in follow-up up till now. Discussion The various types of mural nodules found in the wall of mucinous ovarian tumours include: anaplastic carcinomas, sarcomas of various types, carcinosarcoma, sarcoma-like nodules, mixed nodules, and leiomyomas.[3] Sarcoma-like mural nodules are rare. The last edition of the Armed Forces Institute of Pathology Fascicle for tumors of the ovary indicates that only 16 cases of this lesion had been reported until 1998.[3] Subsequently, 10 additional cases have been reported.[2] Among a few cases described from India, one had features of osteoid-formation within the mural nodule[4] and another showed densely cellular areas with necrosis.[5] The nodules measure up to 6 cm and are usually well circumscribed. Microscopically, they consist of spindle to polygonal cells, osteoclastic giant cells, acute and chronic inflammatory cells. Though pleomorphic cells with bizarre nuclei and mitotic activity (less than ten per ten high-power fields) may be found in these nodules, vascular invasion is typically absent.[3] In our cases the diameters of the nodules were 4 and 4.5 cm, respectively. Whereas in the first case the nodule consisted of spindle shaped cells, multinucleated giant cells, and haemorrhage, the second case showed mostly polygonal cells along with osteoclastic giant cells. In addition to the characteristic features of sarcoma-like nodules, there were many dilated vascular spaces, suggestive of a reactive proliferation.[6] Moreover, cellular features of malignancy such as mitotic activity, cell atypia and vascular invasion were absent. The pathogenesis and nature of these nodules are unclear. They are thought to be reactive and self limited lesions developing in the wall of mucinous cystic ovarian tumours and are associated with a favourable clinical course.[2] The mural nodules probably derive from submesothelial mesenchymal cells as these lesions coexpress vimentin and cytokeratins.[2] The true sarcomatous nodules are usually larger than the sarcoma-like mural nodules, have yellow, pink, or red appearance, and often contain necrotic areas. Microscopically, these lesions may be composed of fibrosarcoma, undifferentiated sarcoma, or rhabdomyosarcoma.[3] Vascular invasion is frequently found.[3] The nodules of anaplastic carcinoma have a diameter ranging from 0.5 to 12 cm and frequently contain areas of necrosis and hemorrhage. The characteristic microscopic features are sheets or nests of large, rounded epithelial cells, having abundant eosinophilic cytoplasm. The nucleus is malignant appearing and the nucleoli are prominent. However, true sarcomatous or carcinomatous nodules when confined to the ovary (Stage FIGO 1A, encapsulated) are not necessarily associated with adverse prognosis.[2] Careful and thorough examination of this uncommon lesion (sarcoma-like mural nodule) within a mucinous cystic tumour is essential for reassuring the patient of a favourable clinical outcome. References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05076f2.jpg] [ms05076f1.jpg] |
| |||||||||

{kind=link}
{kind=link}