 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 59, No. 11, November, 2005, pp. 503-505 Letter To Editor Bilateral hemorrhagic cerebellar infarct in primary antiphospholipid syndrome Udayakumar N, Rajendiran C, Srinivasan AV* Departments of Medicine, *Neurology, Madras Medical
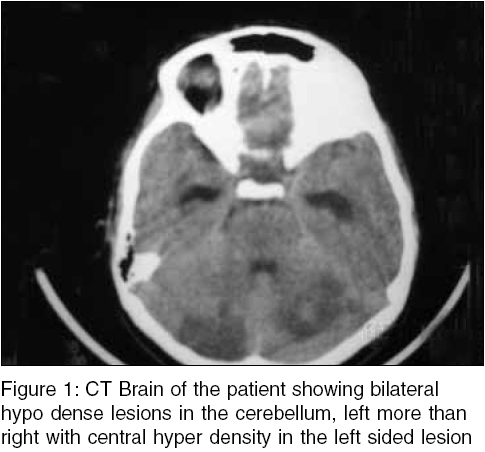
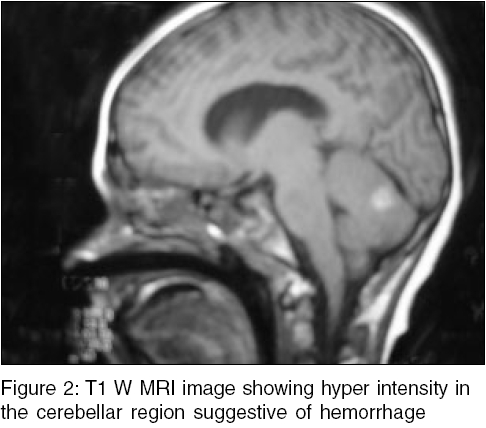
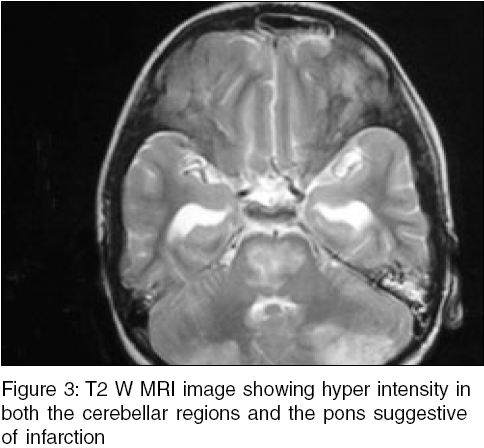
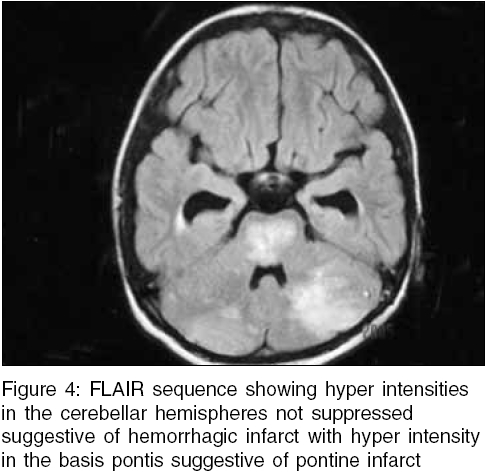
College, Government General Hospital, Chennai, Tamilnadu, India Code Number: ms05077 Ischemic strokes in children are rare[1],[2] and posterior circulation strokes are rarer.[3] Hemorrhagic infarcts of the brain have not been reported in primary antiphospholipid syndrome (APLA). We document the rare instance of bilateral hemorrhagic cerebellar infarction with pontine infarction due to APLA syndrome. A 13-year-old boy presented with bitemporal headache and developed projectile vomiting, became drowsy, unresponsive and admitted to the Intensive care within 2 h. Neurological examination revealed a Glasgow Coma Scale of 4/15. Pupils were equal and reactive to light. Fundi were normal. Plantars were flexor with normal tendon reflexes. The child developed decerebrate rigidity and respiratory arrest requiring endotracheal intubation. Computerized Tomography (CT) of the Brain showed bilateral hypodensities in the cerebellar hemispheres with central hyperdensity, left more than right [Figure - 1]. T1W magnetic resonance imaging (MRI) showed areas of hyperintensities in the posterior cerebellar hemispheres bilaterally suggestive of hemorrhage [Figure - 2]. T2W image showed hyperintensity in both the cerebellar and pontine regions suggestive of infarction [Figure - 3]. The fluid attentuation inversion recovery (FLAIR) sequence also showed hyperintensities in the above regions suggestive of infarction [Figure - 4]. MR Angiography showed enlargement of the proximal portion of the basilar artery with high signal intensity on T1 weighted image suggestive of basilar artery thrombosis with normally paired posterior inferior cerebellar arteries and no evidence of dissection. Cardiac work up including Transesophageal echocardiography, X-ray of cervical spine and metabolic work up were normal. Hematologic work up including Homocysteine, Antithrombin III, Protein C, Protein S, Factor V Leiden, sticky platelet syndrome were normal and Rheumatologic work up including ANA and Lupus Anticoagulant (LAC) were negative. Anticardiolipin antibody IgG was 11.4 GPL units/ml (Normal less than ten) and IgM was 38.1 MPL units/ml (Normal less than ten). This was repeated 6 weeks after the episode that was positive in rising titers, IgM was 51.1 MPL units/ml and IgG was 14.2 GPL units/ml. In children, ischemic stroke is most commonly reported in the distribution of the middle cerebral artery. Posterior cerebral and vertebrobasilar involvement have been distinctly rare.[3] Children unlike adults have some unusually common risk factors for ischemic stroke like infection, trauma, cardiac disease, migraine, sickle cell anemia, and prothrombotic disorders.[4] Our patient was evaluated for all the above said risk factors and based on the clinical and laboratory findings a definite diagnosis of APLA syndrome was made in our patient.[5] Aspirin was withheld in the initial 2 weeks because of the hemorrhagic nature of the infarct, but after 2 weeks the patient was started on low dose aspirin. At discharge, the boy had intact higher functions with minimal cerebellar signs. Prolonged anticoagulation is mandatory in such patients. Warfarin and aspirin have been tried. However, differences of opinion exist on the duration of therapy. Some workers recommend till APLA has been negative for 4-6 months while others suggest life-long therapy. Although rare, this case report highlights the need for emergency room physicians to consider the possibility of Posterior circulation stroke as a cause for unconsciousness in selected subgroups of children References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05077f1.jpg] [ms05077f4.jpg] [ms05077f2.jpg] [ms05077f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}