 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 59, No. 11, November, 2005, pp. 505-507 Letter To Editor Myxoid adrenal cortical carcinoma - A rare variant of adrenocortical carcinoma Suresh B, Kishore TA1, Albert AS1, Joy A1 Departments of Urology, and 1Pathology,
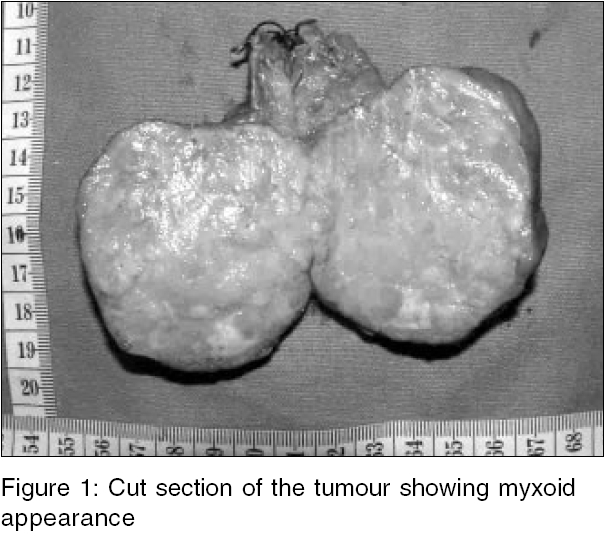
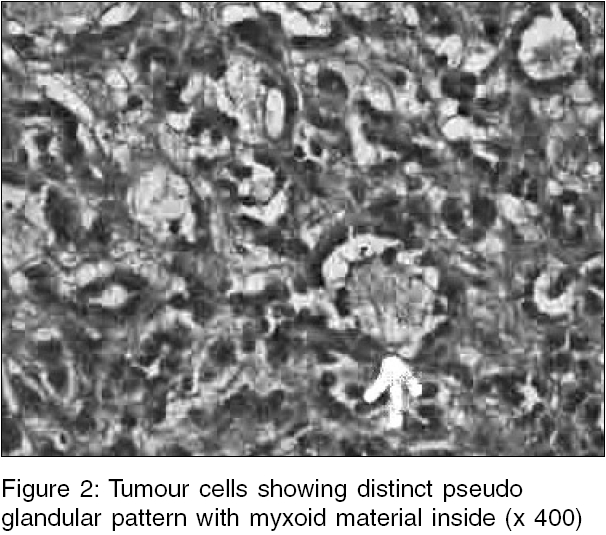
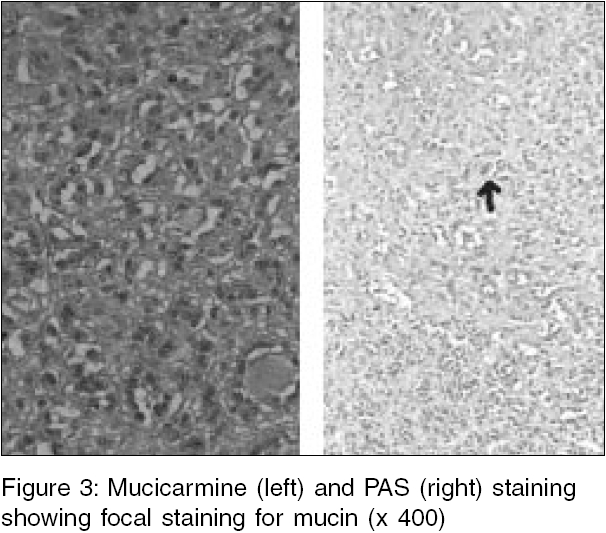
Medical College, Kottayam, Kerala, India Code Number: ms05078 Dear Sir, Adrenocortical carcinomas are malignant neoplasms of the adrenal cortex generally affecting patients in their fourth and fifth decades of life. Myxoid change is a very rare phenomenon in adrenocortical carcinoma, and only 11 similar cases have been reported to date. Myxoid changes in adrenal cortical neoplasm can be present in adrenocortical adenomas also.[1] A 49-year-old male while being investigated for hypertension was found to have right adrenal tumour on ultrasonography. Physical examination was negative There was no hypokalemia and the metabolic workup for pheochromocytoma was negative. Computerized tomography scan revealed heterodense right adrenal tumour of size 6 x 5 cm. There was no evidence of invasion to adjacent structures Right adrenalectomy was performed. The tumour was well encapsulated and resected without any difficulty. Cut section demonstrated circumscribed tumour with uniform myxoid appearance [Figure - 1]. On histopathology examination there were features of malignancy like necrosis, vascular invasion, 4-5 mitotic figures/high power field. The tumour cells showed a pseudo glandular pattern with myxoid material inside [Figure - 2]. Staining done with mucicarmine and Per-iodic acid Schiff (PAS) showed focal staining for myxoid matrix [Figure - 3]. The patient is alive after a follow up period of 1 year with out any evidence of local recurrence and metastasis. Myxoid adrenocortical carcinoma is a rare variant of adrenocortical carcinoma. The presence of myxoid changes in adrenocortical neoplasms usually raises the possibility of malignancy.[1] Tang et al first described this variety in 1979.[2] Myxoid changes have also been reported with adrenal adenoma and these were mostly metabolically normal.[1] The differentiation of benign and malignant tumours can be made by presence of necrosis, vascular invasion, capsular invasion and greater than three mitosis per high power field.[3] The recent literature is replete with articles evaluating the potential role of growth factors, markers of proliferation (Ki 67 and MIB), tumour suppressor genes (p53 Rb-1and p27 and apoptotic regulators (bcl-2) in differentiating adenoma and carcinoma.[4] Some of these may have prognostic value also.[4] The histochemical stains done are Alcian Blue, PAS, Mucicarmine. The histochemical profile of the myxoid material in our study is consistent with that of previous reports.[2],[5] In vast majority of the cases immunohistochemical staining shows vimentin, synaptophysin and inhibin positivity, which is typical of adrenocortical neoplasms.[1] The differential diagnosis of myxoid tumours in retroperitoneum includes chordoma, myxoma, lipoma, liposarcoma, benign and malignant nerve sheath tumours.[2],[5] The 5 years survival rate for malignant myxoid adrenocortical tumour is 50% while that for the adenomas it is 100%.[1] The common sites of metastasis are liver and lungs. Local recurrences have also been reported in 2/10 cases reported previously.[1] References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05078f1.jpg] [ms05078f2.jpg] [ms05078f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}