 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
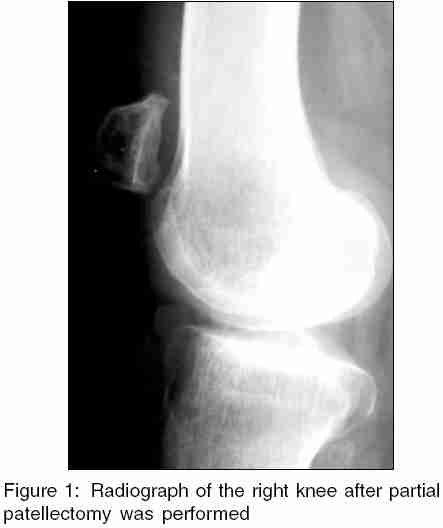
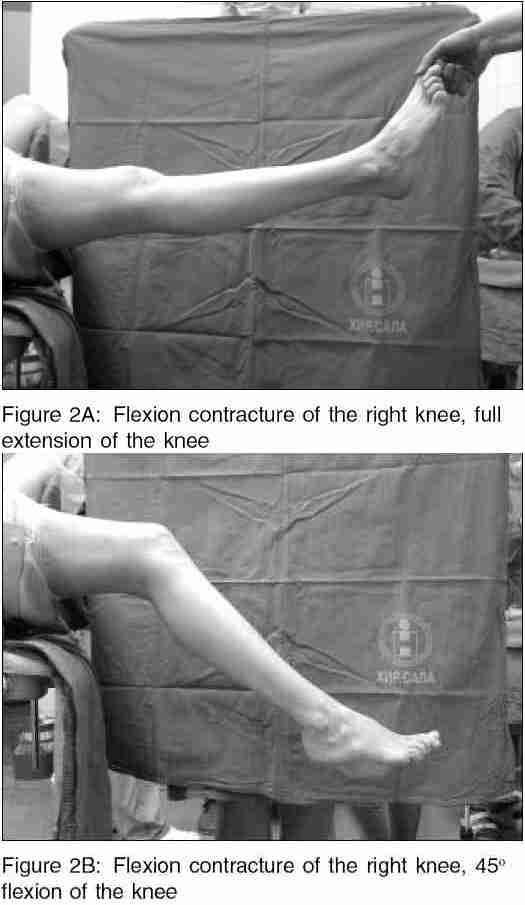
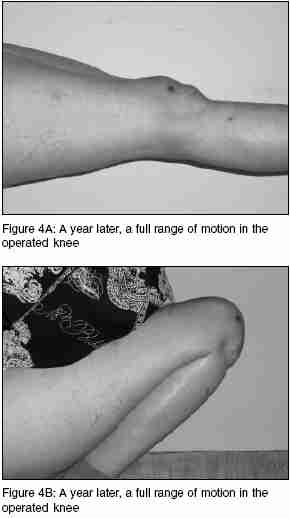
Indian Journal of Medical Sciences, Vol. 59, No. 12, December, 2005, pp. 534-537 Case Reports Treatment of the knee stiffness caused by partial patellectomy; Case report - Technical tricks Milankov M, Miljkovic N, Stankovic M Departments of Orthopaedic Surgery and Traumatology, Institute of Surgery, Clinical Center, Medical School, University of Novi Sad, Hajduk Veljkova, Novi Sad, Serbia and Montenegro Code Number: ms05081 Abstract Partial patellectomy is advised in treating comminuted fractures of patella when accurate reduction and stable fixation cannot be achieved. Usually, after partial patellectomy, the tendon-to-bone junction requires prolonged protection. One of the effects of the prolonged immobilization is lack of knee flexion. Stiffness of the knee was treated with manipulation under anaesthesia. In order to protect patellar ligament insertion to the patella remnant, a Steinmann pin was put through tibial tuberosity, a metal wire was pulled through the patella remnant and tied firmly to the pin. Gentle manipulation was performed and full flexion of the knee was achieved without damaging bone ligament complex.Keywords: Knee stiffness, Partial patellectomy, Treatment Fracture of the biggest sesamoid bone, patella, is encountered at the rate of 1% of all skeletal injuries. Partial patellectomy is advised in the treatment of comminuted fracture of patella when accurate reduction and stable fixation cannot be achieved.[1],[2] Usually, after partial patellectomy, the tendon-to-bone junction requires prolonged protection, which was the recommendation of the most authors in the past. [3],[4],[5],[6],[7] One of the effects of the prolonged immobilization is a lack of knee flexion. A possible way of treating this complication is presented in this paper. Case report - technical tricks A 44-year-old female was brought to the emergency room of a small city hospital after sustaining an injury of the right knee, as a car driver in a head-on collision. Radiographs of the injured knee showed a comminuted fracture of the patella. Following routine preoperative preparations, she was operated in spinal anaesthesia, under tourniquet control. Partial patellectomy was performed [Figure - 1], small bone fragments removed and patellar tendon was repaired by suturing it to the patellar remnant without cerclage wire protection. A cylinder cast was applied postoperatively. Ambulation with crutches began the next day, no weight bearing allowed for the next 6 weeks. After 6 weeks, the cast was removed and the patient was referred to physical therapy, which lasted 2 months. Because of inadequate cooperation between the patient and her physiotherapist, stiffness of the injured knee occurred (range of motion from 0o to 45o of flexion) [Figure - 2]A, B. A lack of knee flexion was treated with manipulation under anaesthesia. In order to protect patellar ligament insertion to the patella remnant, a Steinmann pin (5 mm, diameter 200 mm length) was put through tibial tuberosity, a metal wire (1.5 mm diameter) was pulled through the patella remnant and tied firmly to the pin. Gentle manipulation was performed and full flexion of the knee was achieved [Figure - 3]A,B. All metalwork was removed after manipulation. Continual passive machine (CPM) therapy was started immediately after the operation in the hospital , and lasted for 14 days. It consisted of twice-a-day treatment, each lasting 2 h, followed by passive flexion exercises under physiotherapist supervision. Quadriceps strengthening exercises were introduced simultaneously, as full weight bearing was allowed. Progressive rehabilitation was continued in an outpatient clinic under physical therapy specialist supervision. A year later, on a routine check-up, the patient had a full range of motion in the operated knee, which was equal to the contralateral knee [Figure - 4]A,B. Discussion Comminuted patellar fractures require partial patellectomy in about 20-26% of all patellar fractures.[8] After this procedure, unless the fracture is treated with tension band wiring, followed by early mobilization,[8] a limitation of knee flexion may occur. If this limitation of movement is not dealt with physical therapy in time, the complication becomes a great challenge for treatment.[9] Knee manipulation under anaesthesia carries a high risk of damaging the extensor mechanism. Patellar ligament insertion to the patellar remnant is highly susceptible to avulsion, and, therefore, manipulation under anaesthesia must be performed gently and with great caution. Wong et al.[10] and Leung et al.[11] performed biomechanical tests on bone-tendon junction healing, in a goat and rabbit partial patellectomy model. After 24 weeks, most specimens failed at the junctions under tensile loads. The ultimate failure stress after 24 weeks was 15 and 20.6% of control values. Keeping this in mind during knee manipulation under anaesthesia, we used pin and wire for temporary protection of ligament insertion. In our case, this turned out to be a very successful procedure. References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05081f4.jpg] [ms05081f3.jpg] [ms05081f1.jpg] [ms05081f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}