 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 59, No. 12, December, 2005, pp. 538-541 Case Reports Choriocarcinoma with negative urinary and serum β human chorionic gonadotropin (β HCG) : A case report Mehra Reeti, Huria Anju, Gupta Pratiksha, Mohan Harsh* Department of Obstetrics & Gynaecology, *Department
of Pathology, Government Medical College & Hospital, Sector 32-B, Chandigarh,
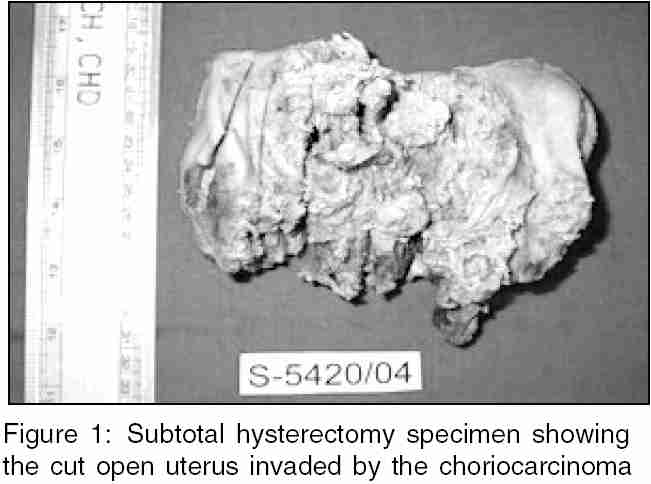
India Code Number: ms05082 Abstract This was a rare case where a patient presented clinically as a case of post abortal sepsis and ultrasound showing the picture of an intramural degenerating fibroid. Her serum and urine both were negative for β human chorionic gonadotropin (βHCG). Patient succumbed to choriocarcinoma 1 month later. Failure to detect urinary and serum βHCG lead to maternal mortality due to the choriocarcinoma. The failure to detect, certain degradation products of HCG which may predominate in gestational trophoblastic neoplasia, by many common HCG testing kits lead to the error of diagnosis. Only 3 of the 7 common commercial serum HCG tests appropriately detects nicked HCG and its free βHCG, DPC immulite assay, being the most sensitive method. Though of rare occurrence, this awareness is important for diagnosis and follow-up of gestational trophoblastic neoplasia and could have been life saving in our case.Keywords: Choriocarcinoma, β Human chorionic gonadotropin (βHCG) assays, Urine pregnancy test Introduction Human chorionic gonadotropin (HCG) tests are the mainstay in the diagnosis of gestational trophoblastic disease (GTD) and very high levels of HCG are of prognostic value as well. In addition to the regular HCG, at least five key variants are present in serum and urine samples: hyperglycosylated hCG, nicked hCG missing the β -subunit, C-terminal peptide, free β -subunit, nicked free β -subunit, and multiple combinations of these variations. All tests, whether radio immuno assay (RIA) or modern immuno-metric assays use at least one antibody directed against the b-subunit and are therefore known as β -hCG test.[1] Some tests may detect regular hCG only, others may detect all seven major hCG related molecules. If a test kit detects only regular hCG, it may not be a problem for testing and monitoring normal pregnancy, however it would be a major problem in monitoring patients with H. mole and choriocarcinoma where one of the hCG variants may predominate. It may also be a problem in cases of GTD in which aberrantly hyperglycosylated hCG,[2] is commonly the principal form of hCG present. Failure to appropriately detect these hCG variants is a common cause of failure to diagnose GTD or its recurrence.[1],[3] A negative urinary and serum β -hCG has been reported in cases of molar pregnancy as well as choriocarcinoma.[4],[5],[6] Recently, Rohit Gutgutia et al. performed a total hysterectomy in a patient with molar pregnancy due to misdiagnosis due to negative urinary and serum β -hCG.[7] Ours was a rare case where presentation was also atypical and failure to detect both urinary and serum β -hCG lead to maternal mortality. Had we asked specifically for DPC Immulite assay to detect serum β-hCG, which is the only test that detects all the variants of β -hCG and also gives the least false positive results,[1],[8] the death may have been preventable. We wish to share our experience with everybody.Case report A 23-year-old lady presented at a private nursing home and was diagnosed to have a missed abortion at 8-week gestation. Evacuation of the uterus was done. Her nausea and vomiting persisted and in addition she started having acute pain abdomen. Keeping a possibility of ectopic pregnancy, a diagnostic laparoscopy was done which showed a small cornual fibroid with pus oozing from it. Serum β hCG was report as less than 5 mI U/ml. Peritoneal lavage was done and patient was put on antibiotics. After another 15 days the patient had high grade fever with signs of acute abdomen and at this point the patient was referred to Government Medical College & Hospital, Chandigarh for further management. On admission the patient was febrile, temperature 39.4°C, anxious, dehydrated with pulse rate of 110/mt and a blood pressure of 100/70 mm Hg. Abdominal examination revealed guarding and rigidity and on pelvic examination exact uterine size could not be made out because of tenderness. Investigations done showed haemoglobin of 9 gm %, TLC 11,000/mm3. Urine examination was normal. Urine for β -hCG by commercially available pregnancy test kit was negative. Ultrasound (USG) showed a normal uterus with endometrial thickness of 7 mm with a subserous fibroid in right cornual region of 5 x 4 cm2 with degenerative changes. There was fluid in pouch of Douglas (POD). Colpotomy yielded 150 ml of thin yellow pus, which grew E. coli on culture. Appropriate antibiotics were given and because of a suspicion of tuberculosis (which is very common in India) an X-ray chest was done. This was normal. The patient responded to the antibiotics and was discharged after 1 week. Repeat serum β -hCG was not done as it is expensive and since urine pregnancy test was negative and a report of serum β hCG done by private practitioner was negative earlier. Placental site trophoblastic tumor was not considered clinically since ultrasound and diagnostic laptroscopy pictures were of fibroid. Also clinically she seemed like post abortal sepsis and responded to the treatment given. She reported to the accident and emergency department after 1 month in shock. Abdominal examination showed uterus to be 24 weeks size and a pelvic examination showed that the cervix admitted one finger and a big submucous fibroid or clotted blood was felt in the cavity of the uterus. USG showed free fluid in peritoneal cavity. A urine pregnancy test was again done by ELISA based commercially available slide kits, which was negative. With a clinical diagnosis of haemorrhage in the fibroid or a leiomyosarcoma, the patient was taken up for laparotomy. At laparotomy it was seen that uterus was replaced by a fungating tumor which had bled intraperitoneally and there was extensive spread to the small intestines and abdomen. To stop the haemorrhage from the fungating tumour, a supracervical hysterectomy was done (see photograph). The patient could not be extubated and was shifted to Intensive Care Unit (ICU). The patient expired on the sixth postoperative day. The histopathology report of the tumor was chorio carcinoma. The pathology department was apprised of the negative urinary and serum β -hCG and were asked to review slides to rule out placental site trophoblastic tumor or leiomyosarcoma but was re-reported as definitely choriocarcinoma. Discussion A negative urine and serum β -hCG pregnancy test is possible in gestational trophoblastic disease if it is secreting principally a variant from of hCG not detected by the routine test for β -hCG. Since urinary hCG was found absent and a report from outside reported negative serum β -hCG also, repeat serum β -hCG, which is an expensive test, was not done. The clinical and ultrasound picture both were atypical in this patient. As high values of β -hCG are the usual clue to a diagnosis of GTD, the diagnosis was missed in this patient. It is important to remember that GTD should be considered in all patients with a preceding history of pregnancy. A biopsy from the growth at the cornu (reported as fibroid) or a fine needle aspiration cytology (FNAC) at the time of ultrasound diagnosis of degenerating fibroid could have aided in the diagnosis. A repeat serum β -hCG specifically by DPC Immulite assay may have helped. Only three of the seven common commercial serum HCG tests appropriately detects nicked HCG and its free β -hCG, DPC Immulite assay, being the most sensitive method.[1],[8][Figure - 1]References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05082f1.jpg] |
| |||||||||

{kind=link}