 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 60, No. 1, January, 2006, pp. 3-12 ORIGINAL CONTRIBUTIONS The impact of HIV/AIDS on the quality of life: A cross sectional study in north India Wig1 Naveet, Lekshmi2 Raja, Pal3 Hemraj, Ahuja4 Vivek, Mittal1 Chander Mohan, Agarwal1 Sunil Kumar 1Department of Medicine, 2Special Care Facility, 3Psychiatry, 4Bipphysics, All India Institute of Medical Sciences, New Delhi, India Code Number: ms06001 Abstract Objective: To determine the impact of Human Deficiency Virus (HIV)/Acquired
Immunodeficiency Syndrome (AIDS) on the quality of life (QOL) on such patients
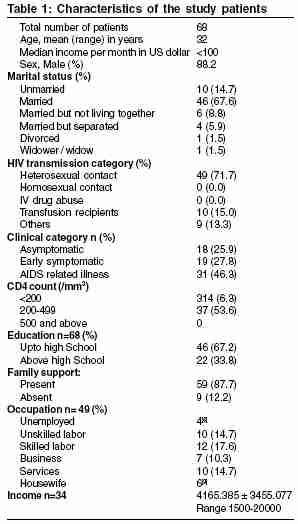
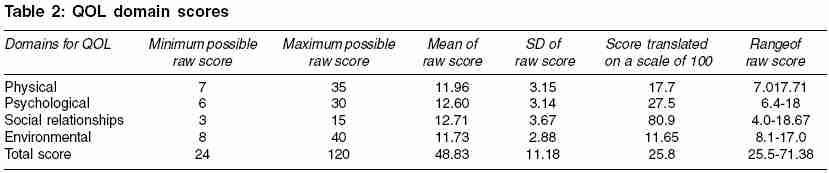
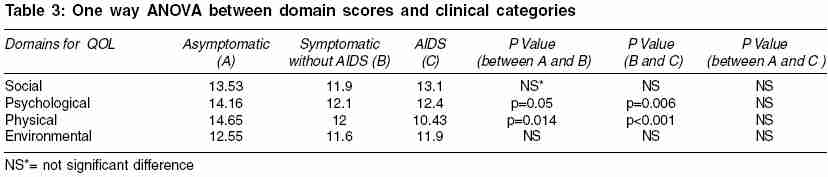
in North India. Keywords: HIV, AIDS, Impact, Quality of life, WHOQOL-Bref Introduction With an alarming increase of Human Immunodeficiency Virus (HIV) /Acquired Immunodeficiency Syndrome (AIDS) in developing countries (estimated prevalence in India=0.91%) and inability to afford highly active anti-retroviral therapy, key issues like the quality of life (QOL) have come to the fore. Determining the impact on the quality of life in HIV/AIDS patients is important for estimating the burden of the disease. This is true because AIDS has a chronic debilitating course and the long-term adverse side effects of current treatments modalities are uncertain. The social stigma attached with the proclamation of HIV sero-positivity may at times force the individual to change the job or the place of living, putting further stress on the already weak economic situation. This further leads to progressive deterioration of health, low morale, repeated consultation, abstinence from work and low productivity. The vicious cycle thus goes on, economic deprivation and social isolation takes it tolls on the quality of life. Quality of life is a multi-dimensional concept whose definition and assessment remains controversial.[1] Quality of life is conceptualized in terms of "an absence of pain or an ability to function in day to day life".[2] Several researchers described Quality of life as a "fighting spirit" associated with longer survival time for individuals.[3],[4],[5] "Quality of life relates both to adequacy of material circumstances and to personal feelings about these circumstances. It includes "overall subjective feelings of well being that are closely related to morale, happiness and satisfaction".[6] Further as health is generally cited as one of the most important determinants of overall quality of life, it has been suggested that quality of life may be uniquely affected by specific disease process such as AIDS.[7],[8] There is lack of clarity in defining Quality of life and concomitant operational difficulties in it.[9] But there is an urgency in evaluating the quality of life in HIV infected individual. Since 1989, more than ten health related quality of life (HRQOL) instruments have been used in research with HIV infected individuals. These have documented relationships of HRQOL and HIV status, level of symptoms, use of antiretroviral drugs and use of drugs for prophylaxis of opportunistic infections separately.[10] This study investigates the quality of life of patients with HIV/AIDS at a hospital based set up in North India. North India is a low risk area for HIV transmission with < 5% high-risk population infected and < 1% Ante Natal Care (ANC) infections. Methods In a cross-sectional study, consecutive HIV/AIDS patients attending Medicine OPD and/or admitted to the wards of All India Institute of Medical Sciences (AIIMS), New Delhi, India were enrolled. Patients visit this hospital from across the country, mainly from the states of Delhi, Haryana, Bihar and Uttar Pradesh. The respondents were evaluated according to a pre-designed protocol. The patients were administered a structured questionnaire by the HIV nurse co-coordinator. The patients filled an additional questionnaire requiring their socio-demographic profile. Informed written consent of all the respondents enrolled in the study was duly taken. Quality of life was evaluated using the World Health Organization Quality of life (WHOQOL) Bref instrument.[24],[25] The WHOQOL Bref consists of 26 items. Each item uses a Likert-type five-point scale. These items are distributed in four domains. The four domains of QOL are, (a) physical health and level of independence (seven items assessing areas such as presence of pain and discomfort; dependence on substances or treatments; energy and fatigue; mobility; sleep and rest; activities of daily living; perceived working capacity); (b) psychological well being (eight items assessing areas such as Affect, both positive and negative self concept, higher cognitive functions; body image and spirituality), (c) social relationships (three items assessing areas such as social contacts, family support and ability to look after family; sexual activity) and (d) environment (eight items assessing areas such as freedom; quality of home environment; physical safety and security and financial status; involvement in recreational activity; health and social care: quality and accessibility). There are also two items that were examined separately: one which asked about the individual′s overall perception of QOL and the other which asked about the individual′s overall perception of his or her health. Domain scores are scaled in a positive direction (Higher scores denote higher quality of life). The mean score of items within each domain is used to calculate the domain scores compatible with the scores used in WHOQOL-100 and subsequently transformed to a 0-100 scale using the following formulas: (Actual raw domain score - lowest possible raw domain score) Where more than 20% data were missing from an assessment, the assessment was discarded. Additionally, where up to two items were missing from a domain, the domain scores was not calculated with exception of social domain, where the domain was not calculated only if ≤1 item is missing. Overall scores could range from a 28 (minimum) to 140 (maximum), with a higher scores indicating better QOL. In contrast to many other quality of life instruments, WHOQOL includes a domain on environment. This is considered necessary as environment plays a major role in determining health status, mediating disease pathogenesis and limiting or facilitating access to health care. Like all other domains in WHOQOL, environmental domain, is also assessed by a subjective self report with the underlying belief that even if subjective reports are at a variance with objective reality, it is the former that determines the quality of life. WHOQOL Bref -a generic instrument could be used in general population to assess a wide range of domains applicable to a variety of health states, conditions and diseases.[11],[12] WHOQOL-Bref Hindi[13] produces an aggregate score and four domain scores instead of individual facet scores. Domain scores produced by the WHOQOL-Bref have been shown to correlate at around 0.9 with the WHO-QOL100 domain scores, and hence provide an excellent alternative to the assessment of domain profile using WHOQOL-100. The bref scale is useful in busy clinics and wards since it takes only 5-8 minutes to complete.[14] There were no patients on antiretroviral drugs during enrollment in the study. Statistical Analysis Results Characteristics of the study patients Heterosexual transmission was found to be the most common. Majority of the patients (53.6%) were in the Category B (CD4: 200-499 cells/ml) while rest of the patients belong to the clinical category C (46.3%): AIDS indicator illness, according to the Centre for Disease Control (CDC) classification (1993 Revised classification system for HIV infection and expanded AIDS surveillance case definition for adolescents and adults). Tuberculosis (38.5%) was the most common HIV related illness, followed by oral candidiasis (28.2%) and then persistent diarrhea (17.9%). The socio-demographic and medical illness related profile of the patients is outlined in [Table - 1]. The mean scores in the four domains of QOL was maximum for the social domain followed by the psychological domain, physical domain and the environmental domain in descending order. QOL domain scores have been summarized in [Table - 2]. The internal consistency between the four domains of the instrument (WHOQOL-Bref) was found to be excellent (Chronbach′s a=0.91). The inter-domain correlation was found positively significant, between all pairs of the four domains using two tailed test at p< 0.001 (Pearson coefficient varied between + 0.52 to + 0.71 between the domain pairs). Physical and psychological domain scores showed significant differences in different clinical categories of HIV patients. However, no significant difference was found between three clinical categories in social and environmental domains. The description of one way Analysis of variance (ANOVA) between domain scores and clinical categories is detailed [Table - 3]. There was no available data for the following socio-demographic categories income (34 patients, which includes housewives) and occupation (19 patients). Level of education of HIV infected individual had a significant effect on psychological domain. A significant difference of quality of life in psychological domain scores was observed between respondents educated till high school and those with education more than high school (p=0.037). However in social domain (p=0.053), environmental domain (p=0.573) and physical domain (p=0.358), there was no significant difference of quality of life between respondents from different levels of education. A significant difference was observed with respect to the occupation of the respondent in the physical domain (p=0.04) and environmental domain (p=0.02). The significant difference of quality of life in physical domain scores was observed between the categories of skilled worker and businesspersons (p=0.02). Additionally in environmental domain too, a significant difference of quality of life was observed between the categories of skilled worker and businesspersons (p=0.03).This may be due to the job security possessed by the businessman as compared to the skilled worker. A significant difference was observed with respect to the income of the respondent in the psychological domain (p=0.048). However, there was no significant difference of quality of life in the physical, social and environmental domains amongst different levels of income. The relationship of scores on domains of WHO-QOL Bref and income were assessed using Pearson′s correlation. No significant co-relations were found. In relation to family support for the patients, a significant difference was observed in the environmental domain. However, there was no significant difference among the respondents for the physical, psychological and social domains. No significant difference was found with respect to the CD4 count in any domain. DISCUSSION WHO has defined quality of life as ′individual′s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns′. Quality of life is often regarded as a concept that is too nebulous to be measured reliably with a structured questionnaire and is subject to too much variability across cultures and individuals to have any useful validity. However, WHOQOL questionnaire developed in the WHOQOL project demonstrated that QOL could be conceptualized and defined in a uniform way across cultures. Its constituent core domains and facets can be assessed using structured questionnaire methodology, and cross-cultural as well as intra-cultural comparisons can be made. WHOQOL-Hindi is available in two versions, the long 100-item version (WHOQOL-100, Hindi) and the brief 26-item version (WHOQOL-Bref, Hindi). Longer version assesses QOL comprehensively while shorter version is most suited for busy clinics. These developments are of major significant to health care professionals, who aim not only to prevent and treat diseases but also to promote health and quality of life. In our study, mean score was highest for social domain in four domains of QOL. Social domain assesses personal relationships, social support and sexual activity. The lack of any significant association on the social domain in this study is in contrast with an earlier study comparing the quality of life in asymptomatic and symptomatic HIV infected patients.[16] The psychological domain accesses the patient′s own thoughts about body image and appearance, negative feelings, positive feelings, self-esteem and personal beliefs. Education, income and clinical categories of patients were found to significantly affect the psychological domain of QOL. The observation of significant difference in the psychological domain in relation to the educational level of more than high school possibly suggests better coping attitudes towards disease. Similarly, higher income of the individual may point towards higher coping capability. Lower psychological domain scores in advanced disease possibly are the reflection of increased morbidity and negative attitude toward life. Earlier reported studies did not compare the impact of education on the QOL in a patient suffering from HIV/AIDS. People in developing countries continue to have low income and are less educated. Disease morbidity usually results in higher deterioration of psychological domain of QOL. Hence decreasing morbidity by easy access to antiretroviral may help in improving psychological domain of QOL. The factors found to have significant affect on the physical health domain were clinical categories and the occupation of individual. The physical health domain assesses the impact of disease on the activities of daily living, dependence on medicinal substances, a lack of energy and initiative, restricted mobility and the capacity to work. As expected, significant difference of quality of life was observed in the physical health domain scores between patients in the clinical categories i.e. asymptomatic, early symptomatic and with AIDS defining illness. It reflects the impact of HIV/AIDS on physical health of the patient as the disease progresses. Skilled workers and businesspersons had better physical health domain scores as compared to others. Suggesting clearly that people with better occupation may have better physical health. This has been documented by earlier studies, that higher levels of symptoms were associated with lower quality of life.[6],[8],[14] There is clearly a need for access to anti-retroviral drugs for all symptomatic patients because lower the morbidity in an individual better is his physical domain score. Environment does play a major role in determining health states. Environmental domain assesses influence of factors like financial resources, the work environment, accessibility to health and social care, freedom, security and participation and opportunities for leisure activities on the QOL. Environment domain had the minimum score in our study. Family support and occupation significantly affected the environmental domain of QOL in our HIV patients. The effect of family support on the environmental domain is a significant observation. Family is usually the most important component of the immediate environment of the patient. The family of the patient can be a major support, in terms of not only financial support, but also safety and security. A good and supportive home environment can help the patient feel better. In addition, skilled workers and businesspersons had better scores in environment domain scores. Hence improving the all round environment surrounding of HIV infected individuals will lead to better quality of life. As documented by the previous studies, treatment has been found to improve the QOL in patients.[23] In our study there were no patients on antiretroviral drugs at the time of enrollment for the study. Better facilities by the government to provide cheaper drugs free of cost for the poor can be a major step in improving their quality of life. In short in our study education, income and clinical categories of the patients significantly affected psychological domain scores. Occupation and clinical categories affected the physical health domain scores. Occupation and family support significantly affected the environmental domain scores. Social domain had the maximum mean domain score and was not significantly associated with any of the determinants. Limitations of the study Conclusions QOL in present study was found to be determined by education, income, occupation, family support and clinical categories of the patients. Family support and occupation provides better environment to individuals suffering from HIV/AIDS. Individuals educated to high school or higher have greater likelihood of possessing better psychological capabilities to cope with disease. Asymptomatic individuals and those who are occupied were found to have a better physical health. However, the results are to be interpreted in the light of small sample size and absence of multivariate analysis. Future directions References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06001t2.jpg] [ms06001t1.jpg] [ms06001t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}