 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
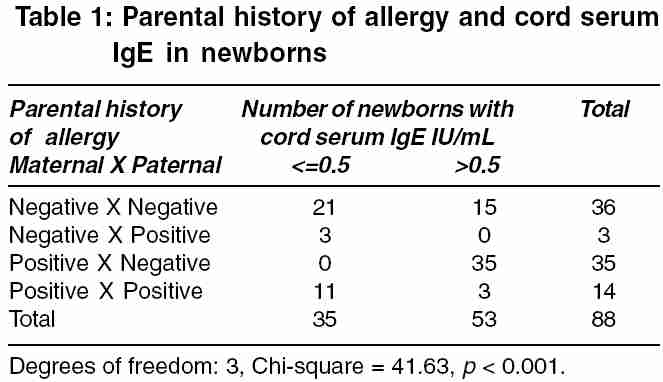
Indian Journal of Medical Sciences, Vol. 60, No. 1, January, 2006, pp. 13-18 ORIGINAL CONTRIBUTIONS Parental history of allergy, maternal serum IgE & cord serum Ige Shah Shilpa, Bapat MM Institute of Science, 15, Madam Cama Road, Mumbai 400 003 Code Number: ms06002 Abstract Background: Allergic reactions are responsible for much illness, irritation and disquiet in the life of the child. Recognition and management of allergy in childhood is of great importance to prevent major allergic syndromes.Aim: To correlate cord serum IgE with parental history of allergy and maternal serum IgE. Settings and Design: In consultation with the attending gynecologist a survey of 950 pregnant women from different parts of Mumbai, visiting gynecology clinics was carried out. Method: 100 pregnant women were randomly recruited for the study. Allergic history of both the parents was collected. Blood samples of mothers and matched cord blood samples were collected. Total serum IgE levels were determined using solid-phase immunoradiometric assay. Total serum IgA from each cord blood sample was checked. Observation & Results: (1) Positive correlation was observed between cord serum IgE and matched maternal serum IgE, with mothers having history of allergy. (2) There was no relation (P=0.99) between cord serum IgE and matched maternal serum IgE, where mothers had no history of allergy. (3) A significant elevation in cord serum IgE was found only with maternal but not with paternal history of allergy. (4) No elevation was found in cord serum IgE (<= 0.5 IU/mL) in 78.6% (11/14) of newborns in spite of both parents having history of allergy. (5) However though there was no parental history of allergy 41.7% (15/36) of newborns showed elevation in cord serum IgE (>0.5 IU/mL). (6) All cord serum samples had IgA<0.06 IU/mL ruling out the possibility of contamination with maternal blood. Conclusion: The maternal history of allergic disease is associated with an elevated cord serum IgE among newborns. Cord serum IgE is a simple, non-invasive and convenient test, which can supplement the maternal history to provide more discriminative information about the allergic status of the newborn. Keywords: Cord serum IgE, Maternal serum IgE, Allergy, Parental history INTRODUCTION "Allergy" is a hypersensitive state acquired through exposure to a particular allergen, re-exposure bringing to light an altered capacity to react.[1] IgE mediated hypersensitivity reactions may cause most allergic diseases. "Atopy" is a type of sensitized state produced by action of the IgE antibody.[2] There is an important inherited component in these diseases is well established.[3] It has now become apparent that inheritance is not a simple, monogenically controlled dominant or recessive pattern. The major problem with incidence and inheritance studies, based on parental history are ascertaining just who should be considered "allergic" or "at risk to become allergic". The reported risk of allergy developing in a child with two allergic parents can be as high as 58 %, when one parent is allergic it is about 29% and a child with neither parents having history of allergy still has about 13 % risk of developing allergic disease sometime during his life.[4] An individuals pedigree can provide useful, but not necessarily conclusive information. Besides, bias from questionnaires of allergic history is also frequently suspected, because a large number of vasomotor rhinitis, intrinsic asthma, and seborrheic dermatitis cases are misinterpreted to be atopic diseases. The risk for development of atopic disease is highest during infancy. Obvious atopic diseases are reported to develop in 12.3 % of the 0 - 1-year-old children.[5] There is a need to implement early-life predictors of allergic sensitization, so that at-risk newborns can be accurately defined and preventive measures instituted. Elevated cord-serum IgE is identified as a marker of later allergic disease in children.[6],[7] The present study was taken up to evaluate it with respect to the parental history of allergy and maternal serum IgE levels. MATERIALS AND METHODS This prospective study was carried out over a period of 1 year (2004-2005). In consultation with the attending gynecologist a survey of 950 pregnant women from different parts of Mumbai, visiting different gynecology clinics was carried out. Using random sampling numbers 100 of them were randomly recruited for the study. The ladies were briefed about the research project and their consent was obtained. Patients′ selection bias was avoided by selecting cases before taking their history. To achieve blinding the maternal & cord blood samples were not categorized as allergic history positive or negative prior to serum IgE estimation. The mothers having the ages of above 18 years were included in the study and the exclusion criteria were pregnancy complications and pre-term or stillbirth. Periodical follow-up of the obstetric check-ups of the recruited subjects was carried out. Blood samples of mothers were collected by vein puncture into plain glass tubes, on getting hospitalized for delivery. Matched cord blood samples were collected in plain tubes immediately after birth, by aspiration from the umbilical vein of the placenta. Total serum IgA from each cord serum samples was checked using Beckman Array 360 system (Beckman coulter, USA). To measure total serum IgE, solid-phase immunoradiometric assay (Diagnostic Corporation Products, USA) with high analytical sensitivity up to 0.08IU/mL, was used. The assay utilized 125I-labelled anti-IgE monoclonal antibodies in liquid phase, and a polyclonal anti-IgE antibody immobilized to the wall of polystyrene tube. During the procedure IgE was captured between the monoclonal tracer and polyclonal antibodies coated to the tube. Decanting and washing the tube removed unbound monoclonal tracer. The tube was counted in a gamma counter for one minute. Total serum IgE concentration was determined by comparing the number of counts with those obtained from the calibrators. The parental allergic history was obtained regarding doctor-diagnosed allergic diseases such as asthma, rhinitis, urticaria, eczema, and anaphylaxis. Statistical analysis: The data was analyzed using Spearman Rank Order Correlation for skewed data and Chi-square Test. RESULTS Out of 100 pregnant women randomly recruited for the study, 12 had pregnancy and/or delivery complications and got excluded from the study. 88 mothers and matched 88 newborns′ cord blood were included for the study. All cord serum samples had IgA < 0.06 IU/mL. The results were categorized depending on the parental history of allergy [Table - 1]. Out of 88 newborns, 36 newborns had no parental history of allergy, 14 had both parents, 35 had only maternal and 3 had only paternal history of allergy. So, in toto 49 (14+35) newborns had maternal history of allergy and 39 (36+3) had no maternal history of allergy. Similarly 17 (14+3) had paternal history of allergy and 71 (36+35) had no paternal history of allergy. 77.6% (38/49) of newborns with maternal, and 17.6% (3/17) of those with paternal history of allergy had an increased cord serum IgE (>0.5 IU/mL). Of the newborns with only maternal history of allergy (n=35) all (100%) had cord serum IgE levels> 0.5 IU/mL. 41.7% (15/36) of newborns without parental history of allergy had an increased cord serum IgE (>0.5 IU/mL). No elevation was found in cord serum IgE (<= 0.5 IU/mL) in 78.6% (11/14) of newborns in spite of both parents having history of allergy. Mothers having history of allergy (n=49) had total serum IgE (median=280 IU/mL, 5-95% values 108-899 IU/mL) significantly elevated (P< 0.001) as compared to that of mothers (n=39) having no history of allergy (median=36.5 IU/mL, 5-95% values 1.35-86 IU/mL). Newborns (n=45) with maternal history of allergy had cord serum IgE (median=0.88 IU/mL, 5-95% values 0.54-3.8 IU/mL) significantly elevated (p< 0.001) as compared to that of newborns (n=39) with no maternal history of allergy (median=0.4 IU/mL, 5-95% values 0.15-0.7 IU/mL). There was significant correlation (Spearman rank order correlation q = 0.27, p = 0.05) between maternal serum IgE of mothers with history of allergy and their matched newborns′ cord serum IgE (n=49). There was no significant correlation (Spearman rank order correlation q = -0.000709, p = 0.99) between maternal serum IgE of mothers with no history of allergy and their matched newborns′cord serum IgE (n=39). DISCUSSION Cord serum IgE is a significant risk factor for the development of allergy in offspring. However, there is a dilemma about its application, with some studies concluding that it is better than family history for predicting sensitization[8],[9] and some that its prediction is not sufficient (low predictive value).[10],[11] The aim of the present study was to correlate parental history and maternal serum IgE with matched cord serum IgE. All our study cord serum samples had IgA < 0.06 IU/ml ruling out the possibility of contamination with maternal blood. The very low cord serum IgE levels even in newborns with raised maternal serum IgE levels indicate that no placental transmission of IgE could have occurred. Maternal IgE antibody does not cross the placenta and umbilical cord serum IgE level is less than 0.5 IU/mL in neonates.[12] It has been reported that the human fetus is capable of producing of IgE from 11 weeks of gestation age and that newborns have a high number of IgE bearing lymphocytes in cord blood.[13] Therefore, it is probable that the IgE in cord blood serum are of fetal origin. 77.6% (38/49) of newborns with maternal, and 17.6% (3/17) of those with paternal history of allergy had an increased cord serum IgE (>0.5 IU/mL) [Table - 1]. The present study confirms the conclusion of earlier studies that it is the maternal, but not the paternal, history of allergic disease which is associated with an elevated cord serum IgE among newborns.[14],[15] Significant correlation (Spearman rank order correlation q = 0.27, p = 0.05) between maternal serum IgE of mothers with history of allergy and their matched newborns′ cord serum IgE (n=49) and no significant correlation (Spearman rank order correlation q = -0.000709, p = 0.99) between maternal serum IgE of mothers with no history of allergy and their matched newborns′cord serum IgE (n=39) is in accordance with the findings of the study by Bjerke et al[16] that negative maternal history and normal maternal IgE levels do not rule out the possibility of sensitization of the newborn. 41.7% (15/36) of newborns without parental history of allergy had an increased cord serum IgE (>0.5 IU/mL), conversely no elevation was found in cord serum IgE (<= 0.5 IU/mL) in 78.6% (11/14) of newborns in spite of both parents having history of allergy [Table - 1]. Since, elevated cord serum IgE increases the risk of allergic sensitization[17] these finding leads to assumption that cord serum IgE estimate, independent of parental history may assist for discriminating sensitization. Strengths of this study include possibility of avoidance of invasive technique of blood collection for total serum IgE estimate in infants and sooner decision about whether the condition is allergic or not, leading to early proper treatment. For parents, knowledge about their infant′s sensitization status at birth can be of importance as regards to the implementation of avoidance measures etc.Limitations of the study are a relatively small sample size, and associated reduction in statistical power. Implementing the test for larger samples with clinical back up along with paternal serum IgE can be future research. CONCLUSION The maternal history of allergic disease is associated with an elevated cord serum IgE among newborns. Cord serum IgE is a simple, non-invasive and convenient test and while there are several ways besides IgE levels to diagnose allergy in the older child and adult, during the first year or two of life, the cord serum IgE record can supplement the maternal history to provide more discriminative information about the allergic status of the newborn.References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06002t1.jpg] |
| |||||||||

{kind=link}