 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
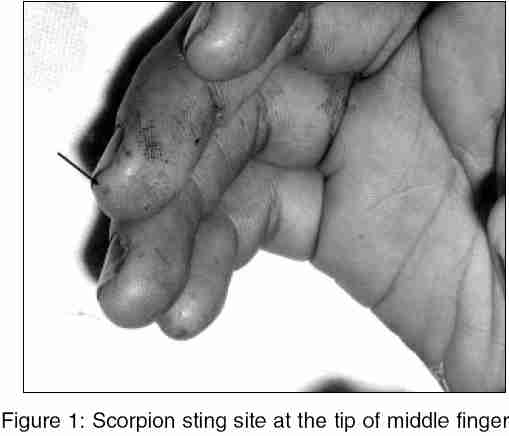
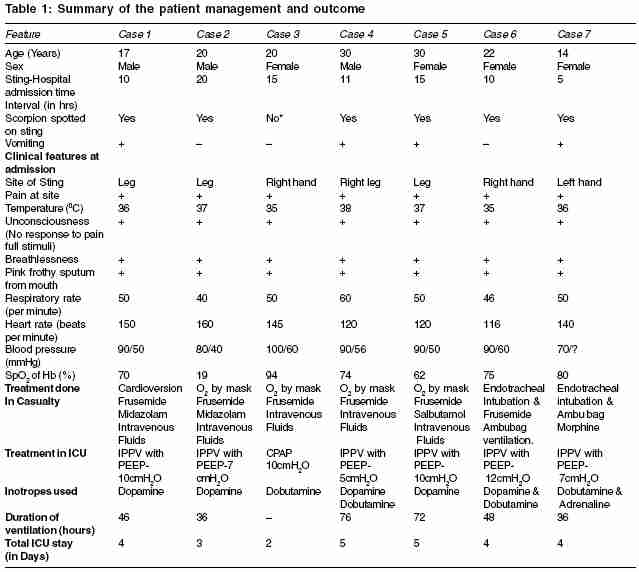
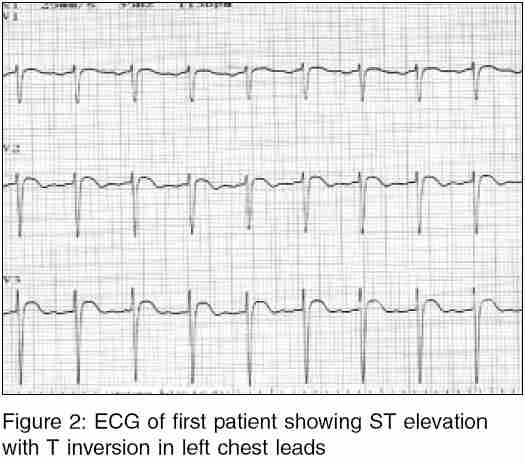
Indian Journal of Medical Sciences, Vol. 60, No. 1, January, 2006, pp. 19-23 Case Report Scorpion sting envenomation presenting with pulmonary edema in adults: A report of seven cases from Nepal Bhadani Umesh Kumar, Tripathi Mukesh, Sharma* Sanjib, Pandey Rajesh Department of Anesthesiology and Critical Care, *Department of Medicine, B. P. Koirala Institute of Health Sciences, Dharan, Nepal Code Number: ms06003 Abstract Scorpion sting is a common problem in villages of Eastern Nepal. The life-threatening complications of myocarditis and pulmonary edema is known in red scorpion in India but not reported in Nepal. This condition requires urgent attention and ICU care from few hours to days. Delay in recognition and the hypoxemia increase the morbidity and mortality. Illiteracy, ignorance, poverty, traditional faith healers trying treatment in remote areas, lack of transport in difficult terrains and the non availability of ventilation facility in nearby hospital, add to delay in appropriate treatment. Seven young adult patients admitted in a span of two years with history of scorpion sting presenting with pulmonary edema required ICU care. They were successfully managed with the positive pressure ventilation with PEEP, cardiac support with inotropes and fluid balance. Magnitude of problem, clinical presentation and management done is emphasized.Keywords: Scorpion sting, pulmonary edema, positive pressure ventilation, inotropes Introduction Scorpion sting is common in rural population of eastern Nepal. Scorpion sting, commonly being less fatal than the snakebite,[1] gets less attention in health setup in this region. Mostly being non-fatal, victims present with mild to moderate symptoms and are attended by the traditional healers in village. Scorpion sting in its severest presentation leads to respiratory distress and mortality is related to development of myocarditis and the pulmonary edema in India.[2],[3],[4],[5] This is the first report of potentially fatal presentation of scorpion sting with pulmonary edema from the eastern part of Nepal having geographical continuity with Indian planes and we wish to share our experience. Case History We received 7 patients in last two rainy seasons in span of two calendar years, presenting with pulmonary edema following scorpion sting. The patients aged (10 to 30yrs) presented in emergency with unconsciousness, breathlessness, cyanosis and pink frothy sputum. The site of the sting and the animals were spotted in all but one patient. The sting marks were remarkable on hands and feet [Figure - 1]. All patients presented with hypotension (mean arterial pressure 49 to 65mmHg), tachycardia (120 to 160), low oxygen saturation (78% to 88%), hypoxemia (PaO2-23.4 to 77.4mmHg and PaO2/FiO2-47 to 162), and the metabolic acidosis (base deficit -2.2 to -9.2) [Table - 1]. After first aid in emergency, all patients were immediately shifted to same ten bedded intensive care unit (ICU) of the university hospital admitting both surgical and medical patients. We monitored patients with intra-arterial blood pressure, central venous pressure, pulse oximetry and the arterial blood gases. Intravenous fluids, sodium bicarbonate to treat acidosis, and inotrope infusion (dopamine/dobutamine) to maintain mean arterial pressure > 60 mmHg. First patient developed ventricular fibrillation in casualty. External cardiac massage, cardiac defibrillation (200, 200 and 300 joules DC shock), intravenous lignocaine (60mg) restored sinus rhythm. Trachea was intubated and positive pressure ventilation with PEEP was started. ECG of the patient showed features of myocardial strain with ST elevation [Figure - 2]. Bedside chest x-ray taken in emergency showed marked bilateral infiltrates suggestive of pulmonary edema. He recovered fully without residual morbidity. Other patients were having similar presentation in emergency with varied severity of pulmonary edema [Table - 1]. With this, other patients were immediately shifted to ICU. Patient No 3, having lower oxygen saturation (94%) and pulmonary edema, the blood oxygenation improved with the use of CPAP mask (10cmH2O) and oxygen inhalation. Six patients required mechanical ventilation between 18 to 48hr. ICU stay lasting 2 to 5 days. Blood stained frothy endotracheal secretions and the bilateral hilar infiltrates in chest X-ray confirmed pulmonary edema in all patients. Other details of patients and the treatment are summarized in [Table - 1]. Discussion The patients presented to our hospital in cardiogenic shock (tachycardia, hypotension and acidosis), respiratory distress (tachypnea), hypoxemia and pulmonary edema. All patients reached 5 to 15h after scorpion sting, as their condition deteriorated at peripheral hospital. Bawaskar and Bawaskar (2000) reported the development of pulmonary edema 4-8 hours after scorpion sting even in hospital settings and recommended early prazocin medication by rural health workers to prevent pulmonary edema.[6] Since these patients presented late, contrary to common presentation of hypertension requiring prazocin,[4] patients had hypotension and hypoxemia. Thus the first line of treatment was respiratory support with CPAP mask in one and intubation with mechanical ventilation in rest. All patients required dopamine or dobutamine infusion to maintain arterial blood pressure> 60mmHg. Patients recovered without residual morbidity with ICU stay from 2 to 5 days. Factors like hypoxemia and hypercarbia contribute to pulmonary hypertension. Hyperoxygenation by positive pressure ventilation at high FiO2 helped to reduce pulmonary hypertension. PEEP helped by alveolar recruitment and by shifting edema fluid away from the alveoli. Hemodynamic control with adequate fluid replacement and inotropic support treated hypotension and improved cardiac function. In severe scorpion envenomation, dobutamine infusion is reported to improve impaired heart function.[7] Antivenom therapy was not used due to non-availability. Besides, recent reports have disfavored its use in preventing cardiovascular manifestations for Indian species of scorpion venom.[8] This report emphasizes the complexity of the clinical picture and the need of intensive approach,[9] based on clinical presentation for excellent results. Scorpion bites are common in Terai ( plains) region of eastern Nepal. The species in these patients was identified as Indian red scorpion (Mesobuthus tamulus ). Indian red scorpion ( Mesobuthus tamulus ) is one of the most toxic envenomation in animal kingdom. Scorpion venom is a species-specific complex mixture of short neurotoxic proteins (31-64 aminoacid sequences), appreciable quantities of serotonin, hyaluronidase and various enzymes that act on trypsinogen.[10],[11] The toxins bind at cell membrane level to the voltage-dependent potassium channels, the calcium activated potassium channel, as well as sodium channels.[11] Autonomic storm, presenting as hypertension, tachycardia and biventricular dysfunction with left ventricular predominance, pulmonary edema and cool extremities,[12] is thus initiated due to alpha receptor stimulation by the toxin. Terminal hypotension could represent catecholamine depletion syndrome or activation of kinin/prostaglandin pathway. These patients were referred from villages situated far away from our hospital. Since majority of scorpion sting present with intense local pain and are non fatal, the victims get injection of local anesthetic around the bite and usually get better after initial sting. These victims, however, developed respiratory distress and were referred late to our center. Since snake bite is considered graver in community than the scorpion sting, the victims get less attention from local health worker and the community. All these factors contributed to delay in reporting at the ICU. Conclusions The reported seven patients represent tip of the iceberg of the problem. True incidence of scorpion sting and its severity is not known in Nepal. Acute myocarditis, cardiac failure and pulmonary edema, still unrecognized, are potentially fatal complication of scorpion sting in foothills of Nepal, having geographical continuity with India. Timely diagnosis of pulmonary edema and the initiation of ventilatory and ionotropic support in ICU was the mainstay in treatment. Proper information about this serious complication of the scorpion-sting amongst the health workers of this region is warranted.References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06003f1.jpg] [ms06003f2.jpg] [ms06003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}