 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 60, No. 1, January, 2006, pp. 25-27 Letter To Editor Pseudo Meigs' Syndrome with benign stromal hyperplasia and elevated CA-125 Mehra Reeti, Huria Anju, Gupta Pratiksha, Harsh Mohan* Department of Obstetrics & Gynaecology, *Department of Pathology, Government
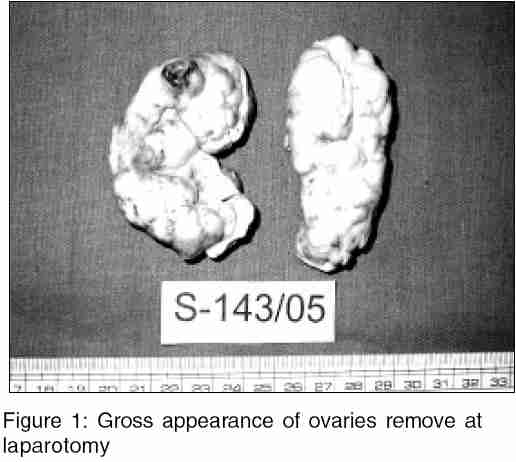
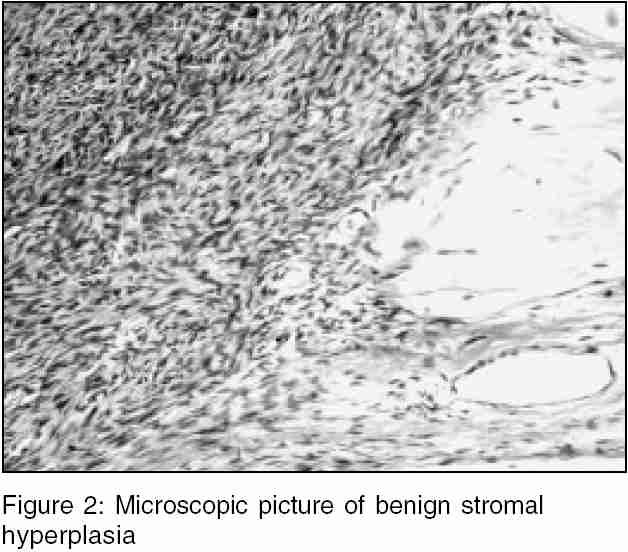
Medical College & Hospital, Sector 32-B, Chandigarh Code Number: ms06005 Sir, We present a rare case of Pseudo Meigs Syndrome associated with benign stromal hyperplasia of ovaries and markedly elevated serum CA-125 levels. A 47 year old perimenopausal lady was admitted in our gynaecology ward with chief complaints of distension abdomen, progressive dyspnoea and pedal oedema for 10 days. There was no other relevant history. On examination she was moderately built and nourished, had massive pedal oedema and was dyspnoeic. She was detected to have reduced breath sounds on the right side of the chest and massive ascites on abdominal examination. On investigations, she was found to be anaemic with a Hb of 8 gm%, hypoproteinemic with a total serum protein of 4.8 gm/dl. X-ray chest revealed right sided pleural effusion. USG and CT scan showed massive ascites and enlarged solid ovaries. No definite mass could be appreciated. Ascitic and pleural tapping was done to relieve her dyspnoea and fluid was sent for cytology and acid fast bacilli. Both were negative for malignancy and tuberculosis. Ultrasound guided fine needle aspiration cytology from ovarian tissue was tried but was not successful. Serum CA-125 was found to be 41,800 mIU/ml. Inspite of tapping five litres of ascitic fluid, patient again developed massive ascites. Our preoperative clinical diagnosis was ovarian malignancy. Due to poor general condition of the patient and likelihood of advanced malignancy, the relatives expressed desire to take away the patient without any surgical intervention. However, since malignancy could not be proved, the relatives were persuaded for allowing surgical exploration. The patient was subjected to exploratory laparotomy, which revealed bilateral solid enlarged ovaries 5 x 4 cms, with nodular bosselated appearance [Figure - 1]. Both ovaries were mobile and total abdominal hysterectomy with bilateral salpingo-oopherectomy was done with infracolic omentectomy and exploration of abdominal cavity was done, which did not reveal any abnormality. Histopathology revealed only a benign stromal hyperplasia of ovaries [Figure - 2]. She came for a follow-up at 6 weeks and three months postoperatively. She was in a satisfactory condition and serum CA-125 levels were found to be less than 5 mIU/ml at 3 months. All her signs and symptoms had regressed. Meigs′s syndrome is the combination of ovarian fibroma, ascites and hydrothorax. The same features when associated with any other solid tumor whether ovarian or uterine is referred to as pseudo Meigs′ syndrome. It may be associated with a malignant ovarian tumour and it may be difficult to say whether the hydrothorax and ascites are due to metastasis or otherwise. Thecomas,[1] sclerosing stromal tumour,[2] and struma ovarii,[3],[4] are benign ovarian tumours which have been reported in literature as causing pseudo-Meigs′ syndrome. All above were also associated with elevated CA-125 levels and became asymptomatic after removal of the ovaries. The origin of the fluid (ascites and hydrothorax) is variously ascribed to as an exudate resulting from mechanical irritation of peritoneum by hard heavy mobile tumour or degeneration in a tumour, active secretion by tumour or changes in capsular veins.[1] In our case both the ovaries were enlarged, solid and nodular. The vascularity however, was normal unlike the sclerosing stromal tumour which is very vascular and appears malignant. Pseudo Meigs syndrome in a patient of systemic lupus erythmatosis without any pelvic mass was reported by Tjalma,[5] where ascites was ascribed either due to filshie clips or as part of Tjalma syndrome. Ours is a rare case and we could not find any such reported in literature with this histopathology. This case also reinforces the non specificity of CA-125 as a marker of ovarian malignancy. There was a strong suspicion of malignancy in this case and relatives were also very keen to avoid surgery. The surgery however, proved to be a boon for a patient. Though a rare entity, one can encounter such cases in clinical practice and this case highlights the limitations of clinical examination, imaging and CA-125 levels and strongly supports that a histopathological diagnosis is a must even when there is a strong suspicion of malignancy. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06005f2.jpg] [ms06005f1.jpg] |
| |||||||||

{kind=link}
{kind=link}