 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
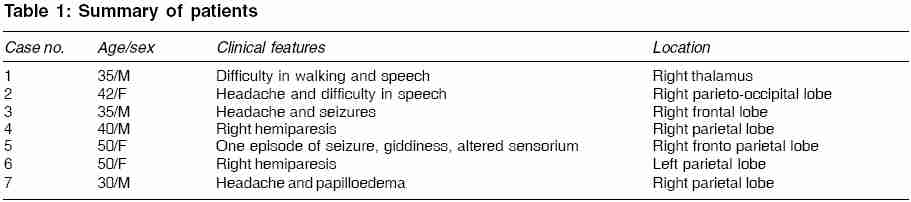
Indian Journal of Medical Sciences, Vol. 60, No. 2, February, 2006, pp. 47-52 ORIGINAL CONTRIBUTIONS Demyelinating disease simulating brain tumours: A histopathologic assessment of seven cases Jain Deepali, Rajesh LS, Vasishta RK, Radotra BD, Banerjee AK Department of Histopathology, Post Graduate Institute of Medical Education and Research, Chandigarh, India Code Number: ms06008 Abstract Background: Demyelinating diseases can present as space occupying lesions with in the brain. It is clinically and radiologically difficult to differentiate them from primary neoplasms. Histopathologically they mimic astrocytic neoplasms closely and identifying these lesions correctly has a profound impact in treatment and prognosis of these patients.Aims and Objectives: The objective was to determine the histopathologic features of such acute focal demyelinating disease that clinically presented as brain tumors. Material and Methods: Seven cases were included for the study. Detailed histopathological examination including stains for myelin and axon were performed. The histopathological keys in arriving at the right diagnoses included a well demarcated lesion that contains uniform distribution of foamy macrophages in the absence of any associated coagulative necrosis, sheets of gemistocytic astrocytes in the white matter that show well-formed processes, perivascular chronic inflammatory cell infiltration and total absence of myelin with relative preservation of axons within these areas. Conclusion: The degree of suspicion (clinical, radiological and histopathological) should be high to diagnose these group of lesions. The above-mentioned diagnostic keys should help in arriving at the correct histopathological diagnoses of such cases. Keywords: Demyelination, pseudotumour, glioma, histopathology Introduction The demyelinating diseases of the central nervous system (CNS) encompass numerous entities, with multiple sclerosis (MS) being the most common among them. These lesions can mimic a CNS neoplasm clinically,[1],[2],[3] on computerized tomography (CT)[4],[5] and on magnetic resonance imaging (MRI).[6] The histopathological findings in tissue samples (biopsies or excisions) of such lesions also can be misleading, that is suggestive of a neoplasm and an incorrect final pathologic diagnosis of "astrocytoma" is offered. The correlation between neuroimaging data and histopathologic diagnosis has been extensively described.[7] It needs to be noted that, it is imperative that clinicians have to be alert to this differential diagnostic scheme. Equally, we also believe, it is important for pathologists to familiarize themselves with this vital diagnostic problem. So this study is aimed at characterizing the histologic features to suspect the diagnosis of demyelinating disease on biopsy and further confirm it with the help of the appropriate special stains. Material and Methods Over the last five years, seven cases could be retrieved from our files, which presented clinically as neoplasm and biopsy confirmed the lesions to be of demyelinating nature. The clinical features of these cases are highlighted in [Table - 1]. All the patients presented with clinical features suggesting a primary brain tumour. There were four males and the average age of presentation was 40 years (range 35-50 yrs). The clinical symptoms ranged from that of increased intracranial pressure to those of weakness and difficulty in speech and mobility. The CT /MRI studies in these patients revealed single lesion in six cases [Figure - 1] and multiple lesions in one case (Case no.3). Glioma (astrocytoma/oligodendroglioma) was the most common clinical diagnosis offered in these cases. Case no.3 had also the differential diagnosis of lymphoma. In all cases surgical intervention was done to achieve a diagnosis, including gross total excisions in some of the cases. Frozen section consultation was carried out in one case (Case no.7) and a diagnosis of glioma was offered per-operatively. In all cases hematoxylin and eosin (H&E) and a myelin stain (Luxol fast blue) was done and Periodic Acid Schiff stain was available in three cases. Immunohistochemistry with Synaptophysin (1:50 dilution) was done in all cases to highlight the axons. Follow up information was available in three of these cases.Results In sections stained with H&E, the most prominent feature of the lesions consisted of collections of numerous foamy macrophages interspersed evenly among the astroglia [Figure - 2]. These collections were sharply demarcated from the surrounding brain parenchyma. Macrophages were strikingly uniform in distribution throughout the lesions, with occasional small focal collections surrounding blood vessels. These foamy macrophages were not associated with areas of necrosis. In Periodic Acid Schiff stain these macrophages showed purple red deposits [Figure - 3]. Admixed with these macrophages were reactive gemistocytes and in one of the case these cells had hyperchromatic bizarre nuclei along with mild vascular proliferation. Myelin stain was negative and disclosed no intact myelin sheaths in any of the cases [Figure - 4]. In contrast to the severe loss of myelin, relative preservation of axons was striking in immunohistochemical staining for synaptophysin. Blood vessels were usually prominent within these areas. Perivascular lymphocytic infiltrate was present in all cases [Figure - 2]. The infiltrate was mild to moderate in intensity. Edema of variable severity and extent was present in three cases. The edema tended to be present in the adjacent brain tissue or at the edge of lesions rather than within the active process itself. There was no evidence of cystic degeneration or presence of Creutzfeldt cells in any of our cases and the adjacent brain parenchyma did not show any significant pathology. Follow up information, available in three of these cases, had the diagnosis of multiple sclerosis substantiated by cerebrospinal fluid electrophoretic examination. All these three patients responded well to steroid therapy (parentral and oral) with remission of their neurological symptoms. Discussion Demyelinating disorders presenting as tumefactive brain lesions pose a diagnostic challenge. From a radiological standpoint, apart from mimicking the appearances of primary neoplasms, they have also been mistaken for abscess and metastatic tumour deposits.[8] Use of serial proton magnetic resonance spectroscopy[9] and repeated conventional magnetic resonance imaging (MRI), 1H-MR spectroscopy and magnetization transfer imaging[10] have proven to be of benefit in distinguishing these lesions. From a histopathologic stand point, the spectrum of various stages in demyelinating diseases are usually classified as active or inactive lesions, based on the presence or absence of inflammation or macrophage infiltration.[11],[12] All our cases showed at least mild perivascular inflammation or macrophage infiltration and can thus all be considered active. Frozen section study is also difficult to analyze[13] as seen in our case, but demonstration of neutral lipid within the macrophages with help of oil red O or other fat stains is helpful. In distinguishing multiple sclerosis from either neoplasia or other non neoplastic processes, the large number and characteristic infiltrative pattern of foamy macrophages is of particular importance. Representing the primary mechanism of demyelination in this disorder, foamy macrophages are dispersed evenly among the astroglia and are not associated with necrosis. Foamy macrophages are occasionally associated with areas of necrosis in malignant gliomas and lipidized tumour cells occur rarely in malignant gliomas[14] or in pleomorphic xanthoastrocytoma.[15] Foamy macrophages, as well as gemistocytic astrocytes, may be numerous in recent cerebral infarction; however, in a sufficiently large biopsy specimen of cerebral infarction, either necrosis or cavitation should be easily identifiable. Also selective destruction of myelin sheaths is not a feature of either a primary brain tumour or cerebral infarction. As pointed out by Zagzag et al,[16] the hypercellularity of the active demyelinating lesion may masquerade as the hypercellularity of neoplastic lesions and the presence of pleomorphic reactive astrocytes with large, often hyperchromatic and even bizarre nuclei often suggests the diagnosis of astrocytomas. The concurrent rare occurrence of demyelinating disease with gliomatous and non-gliomatous neoplasms complicates the picture.[17],[18],[19] Though the neoplastic transformation of reactive glial cells in multiple scleroses plaques has been proposed as the source of gliomas, such association appear to be more coincidental. Gliomas reported in association with multiple sclerosis are more frequently (30%) multicentric than are uncomplicated gliomas.[18] Also it is important for the pathologist to realize that in subacute lesions, inflammation is usually sparse centrally where biopsies are often taken. Regarding the biological behaviour, only exceptionally do such tumefactive demyelinating lesions complicate the course of established disease. The histologic features that form a clue to the diagnosis of demyelination are: presence of foamy macrophages in the absence of any associated coagulative necrosis, presence of a prominent lymphoid inflammatory infiltrate especially around blood vessels, pattern of sheets of well formed large gemistocytic astrocytes with well developed processes that are separated from each other, well defined border of the lesion with predilection for white matter/ periventricular areas.[20] Demyelinating pseudotumour should be considered in the differential diagnosis of any proliferative astroglial process presenting as a mass lesion. With experience, the morphologic features of demyelinating disease are easily recognizable in H&E sections. These features together with further special stains for axons and myelin sheaths help in arriving at the correct diagnosis. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06008f2.jpg] [ms06008f4.jpg] [ms06008f3.jpg] [ms06008f1.jpg] [ms06008t1.jpg] |
| |||||||||

{kind=link}