 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
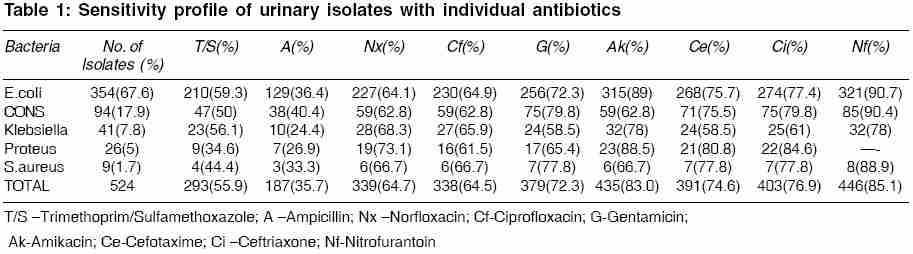
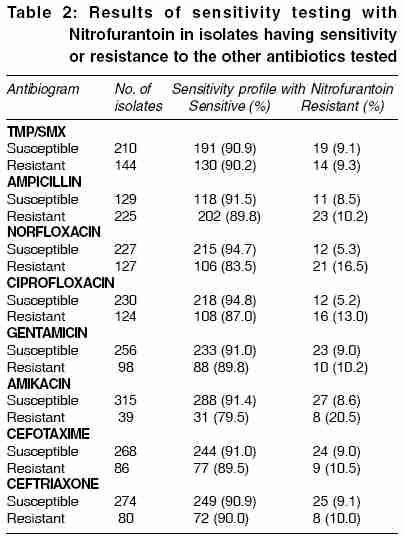
Indian Journal of Medical Sciences, Vol. 60, No. 2, February, 2006, pp. 53-58 ORIGINAL CONTRIBUTIONS Choice of antibiotic for empirical therapy of acute cystitis in a setting of high antimicrobial resistance Biswas Debasis, Gupta Pratima, Prasad Ramjee, Singh* Vikram, Arya Muktanjali, Kumar Ashish Department of Microbiology and Nephrology*, Himalayan Institute of Medical Sciences, Swami Ram Nagar, Jolly Grant, Dehradun, India Code Number: ms06009 Abstract Background: A high prevalence of antimicrobial resistance among urinary isolates in the Garhwal region of Uttaranchal.Aims: To identify the most appropriate antibiotic for empirical treatment of community-acquired acute cystitis on the basis of local antimicrobial sensitivity profile. Settings and Design: A prospective clinico-microbiological study including all clinically diagnosed patients with community acquired acute cystitis attending a tertiary care teaching hospital over a period of three years. Methods and Material: Clean-catch midstream urine specimens, from 524 non-pregnant women with community-acquired acute cystitis, were subjected to semi-quantitative culture and antibiotic susceptibility by the Kirby- Bauer disc diffusion method. A survey was also conducted on 30 randomly selected local practitioners, to know the prevalent prescribing habits in this condition. Statistical Analysis: The difference between the susceptibility rates of E. coli isolates to Nitrofurantoin and the other commonly prescribed antibiotics was analysed by applying the z test for proportion. Results: 354 (67.5%) specimens yielded significant growth of E. coli. >35% of the urinary E.coli isolates were resistant to the fluoroquinolones, which were found to be the most commonly used empirical antibiotics in acute cystitis. Resistance was minimum against Nitrofurantoin (9.3%, 33) and Amikacin (11.0%,39). >80% of the fluoroquinolone-resistant strains were found to be sensitive to Nitrofurantoin. Conclusion: The best in vitro susceptibility profile in our study has been shown by Nitrofurantoin and a significantly high proportion of the urinary E. coli isolates have already developed resistance to the currently prescribed empirical antibiotics, viz. the fluoroquinolones. In view of these in vitro susceptibility patterns, a transition in empirical therapy appears imminent. Keywords: Acute cystitis, Empirical therapy, Antibiotic Resistance Introduction Urinary Tract Infection (UTI) is the third most common cause of hospital visits in our country and[1] perhaps, the commonest cause of office visits by women of reproductive age group. A multitude of factors, viz. the narrow spectrum of bacteria causing community-acquired acute UTI, the severity of the distress, the threat of complications and the absence of culture - sensitivity testing facilities in many places, compel the physicians to start antibiotics empirically. This approach is justified in areas with low prevalence of antibiotic resistance . For example, in the United States, the empiric regimen for acute, uncomplicated cystitis is a 3-day course of double strength Trimethoprim/Sulphamethoxazole (TMP/SMX) in areas where the prevalence of TMP/SMX-resistant pathogens is < 10% .[2] But as this prevalence has exceeded 10-20% in many regions of USA,[3],[4],[5] the current empirical regimen is likely to be replaced by alternative therapies, such as Fluoroquinolones or Nitrofurantoin.[6] Since empirical therapy should be guided by the proportion of pathogens resistant to the chosen antibiotic, the present study was undertaken to determine the sensitivity profiles of urinary isolates in the Garhwal region of Uttaranchal, which would expectedly indicate the most appropriate antibiotic for empirical treatment of this condition. Material and methods This prospective study was conducted on a total of 524 women aged 18-50 years, presenting with uncomplicated, acute cystitis to the Nephrology clinics of a 750-beded tertiary care teaching hospital over a period of 3 years, from June 2000 to May 2003. Consecutive patients who presented with dysuria, frequency, urgency and suprapubic tenderness without associated fever and loin pain during the study period were included in the study. Patients with pregnancy, urologic abnormality, urinary catheterization and hospitalized patients were excluded from the study. Clean-catch midstream urine specimens were collected from every patient and semi-quantitatively cultured using the filter-paper method after obtaining proper informed consent.[7] Inoculation was done on Blood Agar and Mc Conkey Agar plates, which were incubated aerobically at 37 oC overnight. Plates showing growth suggestive of significant bacteruria, with colony counts exceeding 10 5 cfu/ml were subjected to standard biochemical tests for identification and antimicrobial sensitivity testing by Kirby- Bauer disc diffusion method on Mueller Hinton Starch Casein Hydrolysate Agar (Hi-Media laboratories Pvt. Ltd. Mumbai, India).[8],[9] Interpretation as 'Sensitive' or 'Resistant' was done on the basis of the diameters of zones of inhibition of bacterial growth as recommended by the disc manufacturer. While choosing antibiotics for sensitivity testing, a survey was done including 30 randomly selected local practitioners in the neighbouring cities of Dehradun and Haridwar, to know their antibiotic prescription habits in community-acquired acute cystitis. Antibiotics against which sensitivity was tested in the present study included TMP/SMX, Ampicillin, Norfloxacin, Ciprofloxacin, Gentamicin, Amikacin, Cefotaxime, Ceftriaxone and Nitrofurantoin (Hi-Media laboratories Pvt. Ltd. Mumbai, India). Statistical Analysis z test for proportion was applied to determine whether the difference between the sensitivity rates of E. coli isolates to Nitrofurantoin and the other commonly prescribed antibiotics was statistically significant or not. Results The practitioner-survey revealed that ciprofloxacin was the most commonly prescribed antibiotic in this condition, being used by 53.3% practitioners (16/30), followed by norfloxacin (30%, 9/30), TMP/SMX (13.3%, 4/30) and gentamicin (3.3%, 1/30). Of the 524 patients, significant growth of E. coli was found in 354 (67.6%). The other bacteria isolated in our study include Coagulase Negative Staphylococcus (CONS) (17.9%, 94/524), Klebsiella (7.8%, 41/524), Proteus (5%, 26/524), Staphylococcus aureus (1.7%, 9/524). The sensitivity profile of these isolates is shown in [Table - 1]. E.coli isolates were most resistant against Ampicillin (63.6%, 225/354), followed by TMP/SMX (40.7%, 144/354). Similarly, overall resistance rates were found to be highest against Ampicillin (64.3%, 337/524) followed by TMP/SMX (44.1%, 231/524). Nitrofurantoin and Amikacin recorded the least resistance for E.coli as well as for all the urinary pathogens taken together. Difference in the sensitivity rates of E.coli isolates to Nitrofurantoin and each of the commonly prescribed empirical antibiotics was found to be statistically significant (p< 0.01 for Ciprofloxacin, Norfloxacin, TMP/SMX and p< 0.05 for Gentamicin). More than 35% of the urinary isolates were resistant to the commonly prescribed fluroquinolone group of the antibiotics. Since Nitrofurantoin was found to be the most effective antibiotic, isolates sensitive or resistant to the other antibiotics were analysed for their sensitivity to Nitrofurantoin [Table - 2]. Majority of the strains resistant to every other antibiotic was found to be sensitive to Nitrofurantoin. Interestingly, 83.5% (106/127) and 87% (108/124) of the isolates resistant to Norfloxacin and Ciprofloxacin respectively were sensitive to Nitrofurantoin. The rate of Nitrofurantoin-resistance among fluoroquinolone-resistant isolates was 2-3 times higher than that among fluoroquinolone-sensitive isolates. Of the isolates resistant to the different antibiotics, Nitrofurantoin was found to be the least effective against the Amikacin-resistant strains. Eight isolates (2.3%) were resistant to both Nitrofurantoin and Amikacin. Discussion In our study, E.coli isolates accounted for 67.6% of the cases of community acquired acute cystitis, more than 35% of which were resistant to fluroquinolones. Nitrofurantoin was the most effective, not only for E.coli (90.7%, 321/354) , but also for all the isolates combined (85.1%, 446/524). Moreover, 83.5% and 87% of the strains resistant to the empirical antibiotics of Norfloxacin and Ciprofloxacin respectively, were sensitive to Nitrofurantoin. The most suited antibiotic for empirical therapy should have low resistance rates against the potential pathogens, achieve significant urinary concentrations, be cost-effective, be free of adverse effects and satisfy patient compliance. Regarding the acceptable resistance rates, the Infectious Diseases Society of America recommends an antibiotic for empirical therapy only if < 10-20% of the urinary pathogens are resistant to it.[2] This is because in vivo therapeutic results correlate with in vitro sensitivity patterns. [10] Determination of the sensitivity profile of community strains is possible only with periodic surveillance studies. This eco-geographical region of India has a high prevalence of antibiotic-resistant bacteria, which further complicates decisions on the choice of empirical therapy.[11],[12] The maximum antibiotic resistance against Ampicillin and TMP/SMX could be attributed to their wide usage for a variety of indications. Aminoglycosides and third generation Cephalosporins, being injectables, are used restrictively in the community-care setting and, hence have shown better sensitivity rates. Fluoroquinolones have a wide variety of indications, permeate most body compartments and are ubiquitously prescribed, accounting for emergence of resistance. Effectivity of Nitrofurantoin over the fluoroquinolones may be due to the following factors. Nitrofurantoin has a single indication, i.e. acute cystitis, narrow tissue distribution, negligible serum concentration, narrow spectrum of activity, bactericidal activity against E.coli in urine at therapeutic doses and limited contact with bacteria outside the urinary tract.[13] Nitrofurantoin has also been reported to be highly effective against most non- E.coli isolates as has also been found in our study.[14] Karlowsky et al has observed an association between resistance to fluoroquinolones and nitrofurantoin.[6] This observation may hold in an area with low resistance to the fluoroquinolones, whereas in our condition most cases of resistance to fluoroquinolones are secondarily acquired and that is most possibly the reason why we have not observed such association. It has been reported that cure rates with 3-day regimens of Nitrofurantoin are lower than those seen with TMP/SMX or fluoroquinolones[15] and hence 7 days of therapy might be required to achieve higher cure rates.[14],[16] In view of the unaddressed issues of patient compliance to Nitrofurantoin and actual clinical recovery, a large community-based study needs to be done to determine the feasibility of using the drug as empirical therapy of acute cystitis. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06009t1.jpg] [ms06009t2.jpg] |
| |||||||||

{kind=link}
{kind=link}