 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
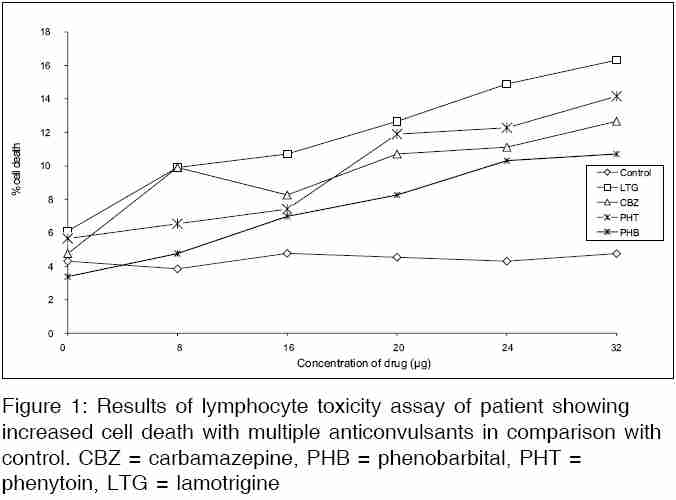
Indian Journal of Medical Sciences, Vol. 60, No. 2, February, 2006, pp. 59-63 Case Report Anticonvulsant hypersensitivity syndrome to lamotrigine confirmed by lymphocyte stimulation in vitro Karande Sunil, Gogtay* Nithya J, Kanchan Sandeep, Kshirsagar* Nilima A Division of Pediatric Neurology, Department of Pediatrics, Lokmanya Tilak Municipal Medical College & General Hospital, Mumbai, *Adverse Drug Reaction Monitoring Centre of Government of India & World Health Organization, Department of Clinical Pharmacology, Seth Gordhandhas Sunderdas Medical College and King Edward VII Memorial Hospital, Mumbai, India Correspondence Address: Sunil Karande Division of Pediatric Neurology, Department of Pediatrics, Lokmanya Tilak Municipal Medical College & General Hospital, Mumbai – 400 022, India E-mail: karandesunil@yahoo.com Code Number: ms06010 Abstract Anticonvulsant hypersensitivity syndrome (AHS) developing to lamotrigine, a non-aromatic anticonvulsant, has rarely been reported. We present a two-year-old boy with refractory epilepsy on valproic acid and lamotrigine therapy who developed fever and a maculopapular itchy rash. Blood investigations detected lymphocytosis and thrombocytopenia. With a presumptive diagnosis of AHS, lamotrigine was discontinued. The fever and rash resolved over the next three days and the child was discharged on valproic acid and clobazam. The diagnosis was confirmed by in vitro lymphocyte toxicity assay, which not only demonstrated increased cell death following exposure to lamotrigine, but also to the three first-line aromatic anticonvulsants: phenytoin, phenobarbital and carbamazepine. The potential of first-line aromatic anticonvulsants to cause AHS should be remembered in a patient who has developed AHS on exposure to lamotrigine. Timely recognition of this rare but potentially fatal drug reaction is important.Keywords: Anticonvulsant hypersensitivity syndrome, Lamotrigine, Lymphocyte toxicity assay Introduction Anticonvulsant hypersensitivity syndrome (AHS) characterized by the triad of fever, skin rash and internal organ involvement is a rare but potentially life-threatening drug reaction that occurs following exposure to an anticonvulsant. [1],[2],[3] Its true incidence is unknown but has been estimated to occur at a frequency of 1/1000 to 1/10,000 exposures. [1],[2],[3] Most of the literature available on AHS is in the form of case reports and case series which has described its occurrence with the first-line aromatic anticonvulsants, viz. phenytoin, phenobarbital and carbamazepine. [1],[2],[3] Cross-reactivity among these aromatic anticonvulsants is known to be as high as 80%. [1],[2],[3] Diagnosis of AHS is difficult because the syndrome occurs one to 12 weeks after exposure to an aromatic anticonvulsant and mimics several infectious, vasculitic and neoplastic conditions. [1],[2],[3] Also, lack of awareness amongst physicians and lack of access to a confirmatory laboratory test contribute to its under-reporting. [1],[2],[3] This article describes a child with refractory epilepsy who developed AHS on exposure to lamotrigine, a non-aromatic anticonvulsant, and the drug reaction was confirmed by in vitro testing. To our knowledge, the present case is the first case wherein in vitro cross-reactivity to the first-line aromatic anticonvulsants was detected while confirming AHS to lamotrigine. Case History A one-and-half-year old male child born of a non-consanguineous marriage was admitted in June 2004 with complaints of multiple (10-15/day) generalized tonic-clonic seizures and regression of milestones since 15 days. His birth and developmental history were normal. There was no history of fever or head injury. Electroencephalogram showed a right-fronto-parieto epileptic focus with secondary generalization. MRI scan showed focal areas of signal abnormality in the left basal ganglia and in cortices of both cerebral hemispheres suggestive of mitochondrial encephalopathy. Metabolic work-up to diagnose the neurodegenerative disorder could not be done as the patient was not affording the tests. To achieve seizure control, the child was given intravenous valproic acid 20mg/kg and oral maintenance dose was gradually stepped up to 40mg/kg/day in t.i.d. doses. After achieving seizure control on day 17 the child was discharged on valproic acid and he remained seizure-free for another one and a half months. In September 2004, the child presented with recurrence of seizures, which were milder in intensity and less frequent (8-10/day). Since lamotrigine is efficacious as an add-on drug with valproic acid for refractory epilepsy, it was started at the recommended low dose of 0.15mg/kg/day and gradually increased to 0.3mg/kg/day in b.i.d. doses after two weeks.[4],[5] The child followed up ten weeks later in December 2004 with complaints of mild to moderate grade intermittent fever since two weeks and skin rash since three days and was hospitalized. The child had continued to have mild seizures (5-8/day). On examination, the child was febrile (39.4oC) and a maculopapular itchy rash was seen on face, scalp and upper chest. Rest of the systemic examination was normal. Blood examination done on admission showed: Hb 12g/dL; total leukocyte count 10.4x10 3/µL with differential count showing lymphocytosis (neutrophils 36%, lymphocytes 64%); and thrombocytopenia (platelets 67.0x10 3/µL). Peripheral blood examination was negative for malarial parasites and atypical lymphocytes. Urine routine examination, liver and renal function tests and chest x-ray were normal. Mantoux test was negative. The patient was managed symptomatically with paracetamol and an antihistamine. Over the next two days, the rash progressed to involve the lower chest, abdomen and the limbs including the palms and soles. On a presumptive diagnosis of AHS, lamotrigine was discontinued. Over the next three days, the fever and rash resolved and the child made an uneventful recovery. The child was discharged after a week on valproic acid and clobazam (0.5mg/kg/day in b.i.d. doses). Two months later, blood sample from the patient was subjected to the in vitro lymphocyte toxicity assay (LTA).[6],[7] The assay demonstrated a higher percentage of lymphocyte death with increasing concentration not only with lamotrigine, but also with phenytoin, phenobarbital and carbamazepine compared with controls [Figure - 1]. In the LTA, at the lamotrigine concentration of 20µg/mL, the percentage of cell death was 12.7%. Maximum cell death (16.3%) was observed at a lamotrigine concentration of 32µg/mL [Figure - 1]. The percentage of cell death in the control sample was 4.5% and 4.8%, respectively, at these drug concentrations. Since it is known that AHS may be genetically determined the mother's and sister's blood samples were collected for LTA.[6],[7] However, their results were nonreactive. The father had deserted the family and could not be tested. Using Naranjo's probability scale for causality assessment a score of 7 was obtained (presence of previous conclusive reports describing similar reaction to lamotrigine, adverse reaction appeared after administration of lamotrigine, increase in the severity of the reaction while the patient was on lamotrigine, adverse reaction improved when lamotrigine was discontinued, absence of alternative causes that could have on their own caused the reaction and the adverse reaction was confirmed by objective evidence) and the reaction was assessed to be "probably" caused by lamotrigine.[8] The child was well on follow-up six months later but continued to have refractory epilepsy. Discussion At initial presentation, as in the present case, AHS may have only two of the classical triad of fever, rash and internal organ involvement.[1],[2],[3] If the offending anticonvulsant is not promptly omitted, single or multi-organ abnormalities occur. The organs involved include the liver (most commonly), bone marrow, lymph nodes, kidney, lung, heart and the CNS.[1],[2],[3] Bessmertny et al[3] in their case series of 14 children with AHS have reported its manifestations in the following order of frequency: fever (100%), rash (100%), lymphocytosis (71%), elevation of liver enzymes (64%), lymphadenopathy (57%), atypical lymphocytes (50%), eosinophilia (43%), coagulopathy (43%), hyperbilirubinemia (36%), leukocytosis (36%), leucopenia (36%) and nephritis (7%). Compared to adults, children may be at a higher risk of development of AHS as the incidence of seizure disorders is higher during the first decade of life.[3] There have been earlier "clinically" diagnosed reports of AHS developing after lamotrigine use: in nine adults and in three children.[9],[10],[11] To our knowledge there has been only one earlier report of lamotrigine-induced AHS which has "objectively" confirmed the drug reaction by the LTA.[12] This recent report has described AHS developing in a 36-year-old man suffering from epilepsy who was concomitantly treated with valproic acid and lamotrigine, as in the present case. But there was no mention of detection of in vitro cross-reactivity of lamotrigine with the three first-line aromatic anticonvulsants.[12] We believe that this finding has important clinical implications as it affects subsequent anticonvulsant treatment options. The potential of first-line aromatic anticonvulsants to cause AHS should be remembered in a patient who has developed AHS on exposure to lamotrigine. The aromatic anticonvulsants are primarily metabolized by cytochrome P450 to reactive arene oxides, which are then detoxified by an enzyme, epoxide hydrolase.[6],[7] It has been postulated that individuals with a deficient activity of epoxide hydrolase develop AHS due to accumulation of arene oxides. These arene oxides are toxic and are responsible for the manifestations of AHS including inducing early lymphocyte death. In the assay, lymphocytes from the patient are used as the substrate and the hepatic microsomes from mice serve as the source of cytochrome P450.[6],[7] However, the pathophysiology of lamotrigine-induced AHS is perplexing as the drug primarily undergoes conjugation and only minor fractions of the drug result in the formation of toxic metabolities.[7] Although the LTA is a diagnostic tool for AHS it cannot be performed during the acute phase because the lymphocyte yield is suboptimal due to death of lymphocytes in vivo and this can lead to increased chances of a false-negative result.[7] Also, the test is conducted in few research laboratories which limits its accessibility to physicians.[7] To conclude, timely recognition of AHS, a rare but potentially fatal drug reaction is important. Discontinuation of the offending anticonvulsant and supportive, symptomatic therapy forms the mainstay of management.[7] Use of corticosteroids and intravenous immunoglobulin in severe cases has been suggested.[7] Once the patient recovers from the acute episode, another structurally dissimilar anticonvulsant should be started. Options available include valproic acid, clobazam, gabapentin, vigabatrin and topiramate.[7] References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06010f1.jpg] |
| |||||||||

{kind=link}