 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
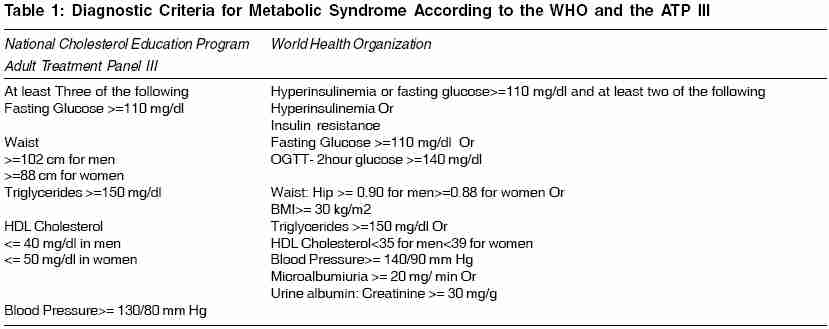
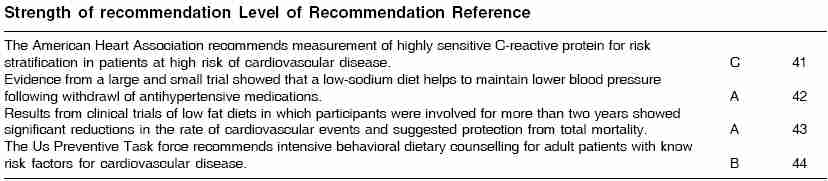
Indian Journal of Medical Sciences, Vol. 60, No. 2, February, 2006, pp. 72-81 Practitioners section Metabolic syndrome Gogia Atul, Agarwal PK Department of Medicine, Sir Ganga Ram, Hospital, Rajinder Nagar, New Delhi-110 060, India Correspondence Address:Atul Gogia, Department of Medicine, J-6/27 Rajouri Garden, New Delhi-110 027, India. E-mail: atulgogs@rediffmail.com Code Number: ms06014 Abstract The Metabolic syndrome is a widely prevalent and multi-factorial disorder. The syndrome has been given several names, including- the metabolic syndrome, the insulin resistance syndrome, the plurimetabolic syndrome, and the deadly quartet. With the formulation of NCEP/ATP III guidelines, some uniformity and standardization has occurred in the definition of metabolic syndrome and has been very useful for epidemiological purposes. The mechanisms underlying the metabolic syndrome are not fully known; however resistance to insulin stimulated glucose uptake seems to modify biochemical responses in a way that predisposes to metabolic risk factors. The clinical relevance of the metabolic syndrome is related to its role in the development of cardiovascular disease. Management of the metabolic syndrome involves patient-education and intervention at various levels. Weight reduction is one of the main stays of treatment. In this article we comprehensively discuss this syndrome- the epidemiology, pathogenesis, clinical relevance and management. The need to do a comprehensive review of this particular syndrome has arisen in view of the ever increasing incidence of this entitiy. Soon, metabolic syndrome will overtake cigarette smoking as the number one risk factor for heart disease among the US population. Hardly any issue of any primary care medical journal can be opened without encountering an article on type 2 diabetes, dyslipidemia or hypertension. It is rare to see type 2 diabetes, dyslipidemia, obesity or hypertension in isolation. Insulin resistance and resulting hyperinsulinemia have been implicated in the development of glucose intolerance (and progression to type 2 diabetes), hypertriglyceridemia, hypertension, polycystic ovary yndrome, hypercoagulability and vascular inflammation, as well as the eventual development of atherosclerotic cardiovascular disease manifested as myocardial infarction, stroke and myriad end organ diseases. Conversely, treatment and consequent improvement of insulin resistance have been shown to result in better outcomes in virtually all of these conditions.Keywords: Metabolic Syndrome, Insulin resistance, Obesity Introduction The 'Metabolic Syndrome' is a widely prevalent and multi-factorial disorder that presents in a distinct, albeit heterogenous phenotype[1] Although obesity and insulin resistance are not synonymous with the metabolic syndrome, they are integral features in this derangement of adipocyte physiology and carbohydrate metabolism. It is now established that this syndrome predicts the development of type 2 diabetes mellitus and cardiovascular disease.[1] Metabolic syndrome was initially observed in 1923 by Kyln, who described the clustering of hypertension, hyperglycemia and gout as the syndrome. Subsequently, several other metabolic abnormalities have been associated with this syndrome, including obesity, microalbuminuria, and abnormalities in fibrinolysis and coagulation.[2] In 1988, Gerald Reaven reintroduced the concept of Syndrome X for the clustering of cardiovascular risk factors like hypertension, glucose intolerance, high triglycerides and low HDL concentration.[3] The syndrome has been given several names, including the 'metabolic syndrome', the 'insulin resistance syndrome', the 'plurimetabolic syndrome', and the 'deadly quartet'.[2] In 1998, WHO proposed a unifying definition for the syndrome and chose to call it the 'metabolic syndrome' rather than the 'insulin resistance syndrome'.[4] This name was chosen primarily because it was the cause of all the components of the syndrome. The Third Report of the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP III) included clinical diagnosis guidelines for the Metabolic Syndrome. Compared with findings from earlier studies and WHO guidelines the new ATP III defines criteria measured in clinical practice[1] [Table - 1]. Individuals who met the criteria for high blood pressure or high fasting glucose concentration if they are currently using blood pressure medications or oral hypoglycemic agents were also included in the definition.[7] European Group for study of Insulin resistance (EGIR 1999) definition for Metabolic Syndrome[5] Insulin resistance (defined as hyperinsulinemia, top 25% of fasting insulin values among the non diabetics population) Plus two or more of the following: 1. Central obesity: Waist circumference> 102 cm (male) > 88 cm (female) Prevalence of Metabolic Syndrome in India and the World With the formulation of NCEP/ATP III guidelines some uniformity and standardization has occurred in the definition of metabolic syndrome and has been very useful for epidemiological purposes. At present, metabolic syndrome is an all or none diagnosis. The study results based on third National Health and Nutrition Examination Survey (NHANES III), indicate that approximately one fourth of the US adults 20 years or older meet the diagnostic criteria for metabolic syndrome.[6] The prevalence of the metabolic syndrome depends on age, ethnic background, and gender. It rises linearly from 20 to 50 years and plateaus thereafter. Looking at various studies around the world, which included population samples, aged from 20 to 25 and upwards, the prevalence varies from 8% (India) to 24% (United States) in men and from 7% (France) to 46% (India) in women.[8] Two Indian studies, which differed in their definition of obesity: first[9] used the obesity criteria suitable for Indians, while the second[10] used the standard ATP III definition of obesity. Both studies used population based samples within the age range but reported prevalence of 13% in Jaipur[10] and 41% in Chennai.[9] The prevalence of obesity in two study groups was quite similar (31% versus 33%), despite the different definitions used. Far larger differences were observed between the two studies for the prevalence of elevated triglycerides (46% vs. 30%), hypertension (55% vs. 39%) and elevated fasting plasma glucose (27% vs. 5%), each of which reported having used the same cut off points. Interestingly, a third Indian study,[11] also from Chennai, reported a metabolic syndrome prevalence of 11.2% (Using EGIR criteria), which was much closer to the prevalence rate reported for Jaipur than the other Chennai study. Therefore, even within the same ethnic population group it appears that there can be significant differences in the prevalence of both the individual factors that constitute the metabolic syndrome and the metabolic syndrome itself. Metabolic syndrome prevalence rates as described earlier vary among ethnic groups as defined by the ATP III criteria among Finnish and Native American men. Both studies involved subjects with comparable age ranges (42-60 and 44-49 years, respectively), with the Finnish study showing prevalence of only 14% compared with the prevalence in the Native American study of 43.6%. The prevalence varies from a low of 13.9% in black men to a high of 27.2% in Mexican American women.[12] Various Factors contributing to increasing prevalence of metabolic syndrome: 1. Atherogenic dyslipidemia, Elevated Triglycerides, apolipoprotein B and small low-density lipoprotein, low HDL. Many studies[15],[16],[17] have reported that low socio-economic status is associated with a higher mortality rate due to cardiovascular disease. A low education level links cardiovascular disease with risk factors such as smoking, hypertension, impaired glucose tolerance, diabetes mellitus, physical inactivity and overweight associated with other metabolic abnormalities. The prevalence of metabolic syndrome was found to be elevated in women who abstained from alcohol.[7] Slight and moderate alcohol consumption has been found to be associated with low CHD risk, possibly through beneficial alterations in HDL cholesterol and blood pressure. Aetiopathogenesis The mechanisms underlying the metabolic syndrome are not fully known; however resistance to insulin stimulated glucose uptake seems to modify biochemical responses in a way that predisposes to metabolic risk factors.[3],[18],[19] A central role has been attributed to the pro-inflammatory cytokines, tumor necrosis factor a (TNF- α ) and interleukin (IL)-6, supported by the fact that both are produced in substantial amounts by human adipose tissue. TNF- α impairs insulin-stimulated glucose uptake in a variety of cells and decreases lipoprotein lipase activity. Both cytokines increase hepatic lipogensis and elicit a systemic acute- phase response.[20] Furthermore, various aspects of the acute-phase response, such as fibrinogen and plasminogen activator inhibitor-1 levels, whole-blood viscosity, and white blood cell count, have recently been found to correlate positively with the metabolic syndrome.[21] This is of particular interest because inflammation plays an important role in the pathogenesis of atherothrombosis.[2],[23] Macrophage and T-cell infiltration is a major feature of atherosclerotic plaques, especially at sites of plaque rupture, and epidemiological studies show strong positive associations of systemic markers of inflammation with atherothrombotic disease.[21],[22],[24],[25],[26] Moreover, C-reactive protein (CRP), the classic and exquisitively sensitive acute phase reactant, shows a strong independent association with the risk of Coronary Heart Disease and other atherothrombotic events. CRP levels have also been found to correlate with BMI and some features of the metabolic syndrome. The AHA/NHLBI/ADA conference identified three potential etiologic categories: 1. Obesity and disorders of adipose tissue 2. Insulin resistance 3. A constellation of independent risk factors (e.g. molecules of hepatic, vascular and immunologic origin) that mediate specific component of syndrome like hypertension, prothrombotic state, lipoprotein metabolic ageing and physical inactivity. Metabolically, several risk factors tend to cluster in middle-aged adults, including HDL-C, BMI, systolic pressure, TGs, glucose and cholesterol.[23] Risk factors occur in isolation only 30% of the time, and clustering of three or more factors occurs 17% of the time in both genders. Clustering of the factors was related to baseline obesity and weight gain during adulthood.[13] Loss of weight over a 16-year period was highly related to a reduced tendency toward clustering of risk factors. In addition, clusters of risk factors were related to greater risk of CHD over the follow up period, and the presence of 3 or more metabolic risk factors led to a doubling of risk for CHD in men and a five-fold increase in risk for women.[13] In Framingham and in other observational studies, the central core of metabolic risk factors were found to be highly related, including triglycerides, HDL-C, BMI, waist circumference, or fasting insulin levels, to insulin levels after an oral glucose challenge test. In addition to a central metabolic syndrome core, there has been a hypertension cluster with shared variance components that included BMI, systolic pressure and diastolic pressure.[13] Clinical Relevance The clinical relevance of the metabolic syndrome is related to its role in the development of cardiovascular disease. Two recent prospective population-based studies confirmed that the metabolic syndrome identified a high-risk group of persons who would have been missed by only consideration of the conventional risk factors. The incidence of coronary disease along with carotid atherosclerosis is higher in patients with metabolic syndrome along with higher mortality from all such causes.[14] Although for many obese patients the risk of developing metabolic syndrome is quiet evident, but studies[4] also show that the risk of having the metabolic syndrome increases steeply even within the overweight or the "preobese" range. Detecting these overweight individuals and the 6% of normal weight individuals with the metabolic syndrome and implementing preventive lifestyle interventions-diet education, physical activity, weight control, smoking cessation, and related behavior modification- is a high clinical priority. Management of metabolic syndrome Treatment strategies Weight gained after the age of 18 years carries a heavy metabolic tag. In the Nurse's Health Study, a weight gain of 10 kg or more since the age of 18 was associated with increased mortality in middle adulthood.[28] The diet advocated by the ATP III panel and the AHA is a modified fat diet. This diet includes 27% total fat content with 8% saturated fats and high pectin containing fruits. The American Heart Association (AHA)[28] espoused an overall healthy eating pattern that would include a variety of fruits, vegetables, grains, low fat or non fat dairy products, fish, legumes and poultry or lean meats and specific guidelines for attaining appropriate body weight, a desirable cholesterol profile, or a desirable blood pressure. Life style Changes Pharmacological Treatment The metabolic syndrome features to be taken care of include atherogenic dyslipidemia, hypertension and insulin resistance. Role of Statins Most high-risk patients who have atherogenic dyslipidemia require statin therapy. Co-administration of drugs targeted for the reduction of LDL precursors (VLDL and IDL) are likely to improve the profile of atherogenic lipoproteins. In addition, co-administration produces a significant rise in HDL cholesterol.[31] Although fibrates reduce plasma triglycerides by 30%-50% and increase HDL by 10% to 15% when used in patients with type 2 diabetes, but there have been no studies specifically examining the effect of fibrate treatment in patients with metabolic syndrome.[31] Role of Aspirin in treatment of metabolic syndrome Primary prevention Role of Glitazones All available evidence on surrogate markers suggest that glitazones have effects to decrease the negative manifestations and risk factors associated with insulin resistance, in individuals with or without diabetes. In the absence of outcome data, it is not possible to make a recommendation for the use of glitazones in clinical practice except for the treatment of type- 2 diabetes mellitus. Hypertension management NHANES III data shows that upto the age of 60 years, higher the BMI, the greater the prevalence of hypertension. The Normative Aging study demonstrated that diastolic blood pressure is a function of increasing abdominal girth.[34] Increases in abdominal circumference are particularly concerning in individuals with a BMI range of 25 to 30; in these individuals, the opportunity to improve blood pressure with small amounts of weight loss should not be missed. When weight loss occurs in obese adolescents and adults with hypertension, a significant relation between improvement in insulin sensitivity and a decreased blood pressure can be seen. It has been estimated that 50% of hypertensive patients are insulin resistant and hyperinsulinemic.[35] The Dietary approaches to Stop Hypertension (DASH) trial has shown convincingly that a healthful dietary patterns can favorably influence elevated blood pressure even without sodium restriction.[36] The DASH trial diet is high in fruits, vegetables, low-fat dairy products, whole grains, poultry, fish and nuts, which are good sources of potassium, calcium, and magnesium and low in fats, red meat and sweets.[37] Treatment of Hypercoagulability / Inflammation Ridker et al[38] found that among 14,719 healthy women followed up prospectively, as the number of risk factors for the metabolic syndrome increased, the levels of C- reactive protein (CRP) increased. Exercise plays an important role in combating this unwanted aspect of metabolic syndrome. A survey of 3800 British men showed that whether they had CHD or not, physical activity showed a significant and inverse dose-response relationship with fibrinogen, plasma and blood viscosity, platelet count, coagulation factors VIII and IX, von Willebrand factor, fibrin-D-dimer, tissue plasma activator antigen, CRP and white cell count, even after adjustment for possible confounders.[39] In addition, a study of obesity-related inflammatory markers and leisure time activity indicated a beneficial effect of frequent physical activity.[40] Prevention The USPSTF recommends intensive behavioral dietary counselling for adult patients with known risk factors for cardiovascular disease.[44] The diabetes prevention programme[45] demonstrated that vigorous lifestyle intervention in patients who are pre-diabetic could reduce the rate of developing diabetes by> 50% (from 11% to 4.8%) Summary 1. Metabolic Syndrome is one of the commonest risk factors for Cardiovascular mortality.2. The major characteristics of metabolic syndrome include insulin resistance, abdominal obesity, elevated blood pressure and lipid abnormalities. 3. Currently, no randomized controlled studies are aimed specifically at treating metabolic syndrome. 4. The primary goals of dietary management for persons with metabolic syndrome are to reduce the risk of cardiovascular disease and diabetes mellitus. 5. The long term effects of low-carbohydrate diets have not been studied adequately in patients with metabolic syndrome, although short-term effects show benefit[Tabel 2]. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06014t2.jpg] [ms06014t1.jpg] |
| |||||||||

{kind=link}
{kind=link}