 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
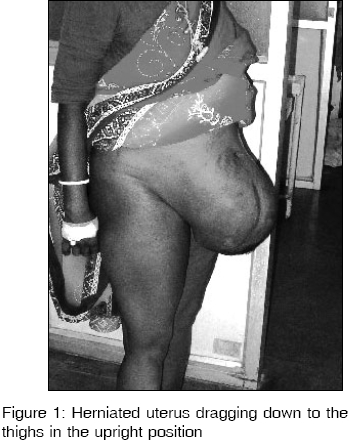
Indian Journal of Medical Sciences, Vol. 60, No. 4, April, 2006, pp. 154-157 Case Report A case of herniated gravid uterus through a laparotomy scar Rao Radha S., Shankaregowda H.S. Department of Obstetrics and Gynaecology, Bangalore Medical College, Fort Road, Bangalore - 560002, India Code Number: ms06023 Abstract A 36-year-old manual worker presented in her second pregnancy at 34 weeks of gestation with an unusual bulge of her abdomen. The lower abdominal bulge turned out to be her gravid uterus herniated through an anterior abdominal wall incisional hernia which is a rare but serious obstetric situation with complicationssuch as premature labour,intrauterine growth retardation, strangulation, intrauterine death and rupture of the lower uterine segment been reported. We had a successful outcome by conservative treatment till 38 weeks of gestation followed by an elective lower segment Caesarean section with hernia repair. Incisional hernia is a frequent complication of abdominal wall closure and the management of pregnancy with a large incisional hernia with gravid uterus in its sac is challenging.Keywords: Herniated gravid uterus, incisional hernia, hernia repair, caesarean section. Introduction A rare but serious obstetric situation can present when a gravid uterus herniates into an anterior abdominal wall incisional hernia.[1],[2],[3] It is potentially a grave obstetric situation with serious maternal and foetal risks such as incarceration, strangulation, rupture of lower uterine segment and other complications. Here we report a case where a woman presented with the pregnant uterus herniated through the anterior abdominal wall incisional hernia at 34 weeks of gestation. A literature search revealed five such cases ever reported in the past.[1],[2],[3],[4],[5]Case Report A 36-year-old woman manual worker presented to us at 34 weeks of gestation with an unusual bulge of her abdomen reaching down her thighs on standing with ulceration over it. She also had discomfort and dragging sensation since a week previous to admission. She was referred to our hospital from a rural area and was unbooked. She had a normal vaginal delivery five years previously with no antenatal or postnatal complications. She had undergone a laparotomy 3 years previously for an ovarian tumour following which there was wound infection and which was treated by antibiotics. On general physical examination, she was moderately built and nourished and appeared mildly pale.She was afebrile with stable vital signs. [Figure - 1] Her lower abdomen was distended mainly below the umbilicus, which also showed a broad vertical paramedian scar and a pressure ulcer of about 4 x 4 cm with surrounding skin showing ischemic changes [Figure - 2]. Fetal parts were easily felt with fetal head in the lower pole and unengaged. Haemogram and urine examination were normal. Ultrasound scan revealed the uterus to have herniated in the incisional hernia of the anterior abdominal wall and a single live fetus in longitudinal lie with average liquor with no gross congenital abnormalities and with placenta in the upper uterine segment was detected. The patient was treated conservatively with rest, binders and daily wound dressing with antiseptics. She was monitored with daily fetal movement counts, weekly CTG and a repeat scan after 3 weeks which revealed satisfactory growth. However due to worsening downward distention in the upright position, she was taken up for elective lower segment Caesarean section at 38 weeks of gestation under spinal anaesthesia. A sub-umbilical transverse elliptical incision was made on the abdomen and the ulcer was removed with the redundant skin. The gravid uterus was immediately under the skin and a live female baby 2.75 kg was extracted through a transverse incision on the lower segment of uterus. The baby had APGAR score of 7 at 1 minute and 9 at 10 minutes and did well. Syntocinon 5 IU was given after placental delivery and bleeding was within normal limits. The hernia was repaired using a 15 x 7.5 cm size polypropylene prolene mesh, which was anchored using circumferential horizontal mattress sutures under the rectus sheath. The patient was covered with antibiotics for a week and did well postoperatively and went home on the eight postoperative day and on follow up at 6 weeks was doing well. Discussion The presence of a gravid uterus in an anterior abdominal wall incisional hernia can pose a serious obstetric situation, which requires emergency reduction. A case has been described as early as 1977 when a woman presented with pressure necrosis of a caesarean section scar with protrusion of the gravid uterus through the wound.[3] There have been reports of problems of prolonged hospitalization due to ulceration on the anterior abdominal wall, preterm labour, intrauterine growth retardation, accidental haemorrhage, strangulation, intrauterine death, rupture of the lower uterine segmentand other complications.[4],[5] There was no post partum hemorrhage in our case but there have been reports of Caesarean hysterectomy, primary post partum hemorrhage and death in the literature.[3],[4] Due to lax abdominal wall and decreased positive intra-abdominal pressure, the effect of the usual dose of spinal anesthesia was anticipated to be unpredictable but there were no problems encountered in our case. Infection and malnutrition along with poor surgical technique have played a role in the aetiology of incisional hernia in this patient. Incisional hernia is a frequent complication of abdominal wall closure with a reported incidence of between 5% and 15% following vertical midline incisions at one-year follow-up.10 With Caesarean section rates showing a rising trend, we have to reflect on its long-term complications and its impact on future pregnancies.[8] The incidence of incisional hernia has been reported to be 3.1% following Caesarean sections and was found to be associated with midline incisions, the need for additional operative procedures, antibiotic administration longer than usual with more potent antibiotics, presence of postoperative abdominal distension, intra-abdominal sepsis, residual intra-abdominal abscess, wound infection, wound dehiscence and postoperative fever.[6] Though herniorrhaphy can be performed during pregnancy if there is necrosis of the skin or risk of morbid incarceration, it is usually postponed until delivery as the enlarged uterus may interfere with healing. We chose to repair the hernia during the operation for Caesarean section as has been done in some previous reports but delayed mesh repair after 6-8 weeks was another option that was considered in view of risk of bleeding and infection.[1] The total recurrence rate following Mayo overlap has been found to be 37%, in contrast to 15% after mesh implantation and therefore is the chosen method of repair.[7] The management of incisional hernia in pregnancy is mainly conservative. A Caesarean section in a woman with large incisional hernia offers a means of hernia repair during the operation while a vaginal birth provides time for healing and a delayed repair to be scheduled. Vaginal birth after Caesarean section with an incisional hernia raises questions about wound integrity and hence is an issue that needs to be addressed in such women who present in spontaneous labour. We have found no literature regarding the subject of management of women with mesh repairs in subsequent pregnancies and needs looking into. We wish to highlight that the clinical awareness of herniated gravid uterus in an incisional hernia sac, which is a delayed, but rare complication of an abdominal wall closure will prevent delay in its diagnosis and treatment[9]. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06023f1.jpg] [ms06023f2.jpg] |
| |||||||||

{kind=link}
{kind=link}