 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 60, No. 4, April, 2006, pp. 159-161 Letter To Editor Extranodal non-Hodgkin's lymphoma of the parapharyngeal space Sajid S. Qureshi, Tanuja M. Shet*, Ganesh Nagarajan, Anil K. Dcruz Department of Surgical Oncology, *Department of
Pathology, Tata Memorial Hospital, Ernest Borges Road, Parel, Mumbai,
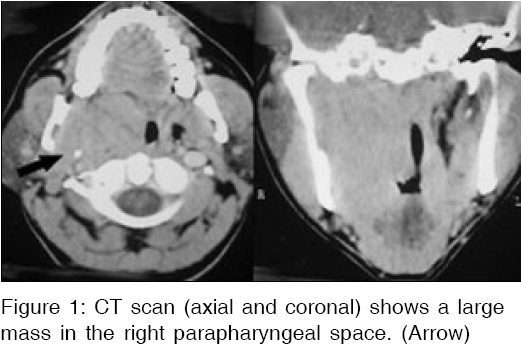
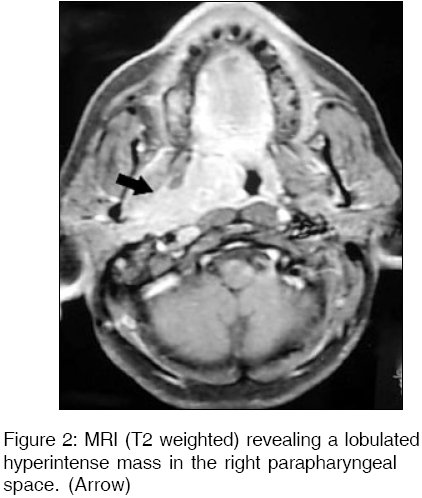
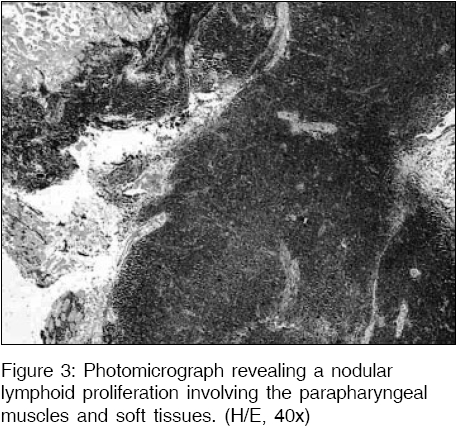
India Code Number: ms06025 Sir, A 40-year-old male presented with diminished hearing, occasional tinnitus and intermittent pain in the right ear of two-year duration that was gradually increasing. Intraoral examination revealed a large right paratonsillar bulge pushing the entire tonsil towards the midline, which was normal on palpation. Parotid gland was normal and there was no appreciable cervical lymphadenopathy. Computed tomogram scan revealed a right parapharyngeal space (PPS) mass involving the nasopharynx and oropharynx. [Figure - 1] The medial and lateral pterygoid plates were eroded and minimal infratemporal fossa infiltration was present. Magnetic resonance imaging revealed a large lobulated hyperintense mass on time (T) 2 weighted images in the PPS extending from the skull base to the level of the mandible. [Figure - 2] Fine needle aspiration cytology (FNAC) was inconclusive. On exploring the PPS a diffuse mass filled the entire PPS with indistinct planes with the adjoining structures. The palatine tonsils however appeared separate from the mass. A biopsy of the mass was performed which on frozen section examination was suspicious of a low-grade lymphoma and hence further excision was not performed. The final histology revealed atypical lymphoid cells forming nodules and involving the parapharyngeal muscles and soft tissues. [Figure - 3] The cells were CD20 and Bcl2 positive and CD43, CD3, CD5, CD23, CD10 negative. Based on the immunohistochemistry and morphology a diagnosis of extranodal marginal zone NHL was made. After relevant staging investigations patient was grouped as stage II EA and received six cycles of adriamycin, cyclophosphamide, vincristine and prednisolone (CHOP) chemotherapy, followed by radiotherapy (46 Gray in 23 fractions over 32 days). At two-year follow-up the patient is asymptomatic and was controlled clinically. Only 10% of patients with NHL present with extranodal disease in the HN sites.[1] Primary malignant lymphomas of the PPS are rare and reported in the literature as isolated case reports or part of larger series of parapharyngeal space tumors.[2],[3] These extranodal NHL are predominantly B-lymphocyte origin and only 11% are low grade.[4] Distinction of lymphomas from carcinomas and other cancers of the head and neck are critical in designing treatment. There are no pathognomonic radiological features of PPS lymphoma however imaging is useful in excluding other common tumours of the PPS. FNAC does not contribute significantly to the differential diagnosis of parapharyngeal lesions. Patients with localized (Stage I and IE) extranodal NHL are treated primarily with radiotherapy. Those with Stages II to IV receive combined chemotherapy and radiotherapy. Surgery has been limited to use in establishing the diagnosis.[5] The overall 5-year and relapse free survival is 60% and 50% respectively.[5] References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06025f3.jpg] [ms06025f1.jpg] [ms06025f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}