 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
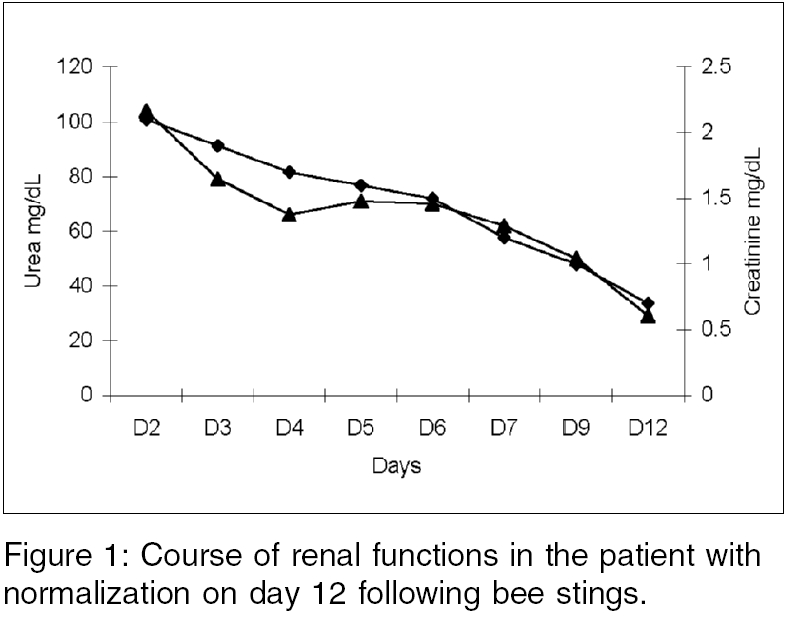
Indian Journal of Medical Sciences, Vol. 60, No. 5, May, 2006, pp. 202-204 Letter To Editor Acute renal failure following multiple honeybee stings Sanjay Vikrant, Ramesh Kumar Patial* Departments of Nephrology and Medicine*, Indira Gandhi Medical College, Shimla, Himachal Pradesh - 171 001, India Departments of Nephrology, Indira Gandhi Medical College, Shimla, Himachal Pradesh - 171 001 Code Number: ms06030 Sir, Stinging events involving honeybees and wasps are rare; most deaths or clinically important incidents involve very few stings (< 10) and anaphylactic shock. However mass stinging events can prove life threatening via toxic action of the venom when injected in large amount.[1] Several types of uncommon reactions have been described including serum sickness, renal diseases, respiratory and neurological manifestations, hepatic dysfunction and delayed hypersensitivity phenomena.[2] We report a rare cause of acute renal failure following rhabdomyolysis and hemolysis due to multiple honeybee stings. A 60 years old female was stung by a swarm of honeybees (forest bees, Apis dorsata) one day previous while she was collecting fodder in the forest. She was initially treated at district hospital and referred because she developed hematuria and decreased urine output. On examination, patient was conscious and oriented. There was swelling of the face. Pallor and dehydration was present. She was hemodynamically stable. She had multiple sting marks all over body (~200), skin was infiltrated by edema and stung areas were edematous and erythemaous. No abnormality was found on systemic examination. Her investigations revealed: Hemoglobin 10.5g/dL, total WBC count 5200, Platelets 150x10 9/L, Peripheral smear showed reticulocytosis and polychromatic RBCs. Blood urea 104 mg/dL, creatinine 2.1 mg/dL (normal 0.5-1.5), sodium 137 meq/L, potassium 5.4 meq/L, calcium 8.5 mg/dL, phosphorous 6 mg/dL, uric acid 7.5 mg/dL, protein 5.2 gm/dL, albumin 3.5 gm/dL, bilirubin 1.5 mg/dL (conjugated 0), aspartate aminotransferase (AST) 121 IU/L, alanine aminotransferase (ALT) 149 IU/L, alkaline phosphatase 112 U/L, lactate dehydrogenase (LDH) 2740 U/L (normal 240-480), creatine phosphokinase (CPK) 2888 U/L (normal< 167). Arterial blood gas (ABG) revealed pH 7.35, paO 2 80 mmHg, paCO 2 34, HCO 3 18 meq/ L. Urine examination: albumin +, pus cells 8-10 /hpf, RBCs 6-8/hpf, urine hemoglobin +, urine culture - sterile. Fractional excretion of sodium (FENa) 5%. Laboratory findings were consistent with intravascular hemolysis, rhabdomyolysis, acute renal failure and hepatic dysfunction. Patient was treated with I. V. fluids, diuretics, antibiotics, steroids, antihistaminic and sodium bicarbonate. This led to improvement in urine output and there was a gradual improvement in renal functions. The patient did not require dialysis and renal function test (RFT) normalized on day 12 [Figure - 1]. This case demonstrates that multiple bee stings may cause rhabdomyolysis and hemolysis with consequent ATN. Components of venom responsible include toxic surface-active polypeptides (mellitin and apamin), enzymes (phospholipase A 2 and hyaluronidase) and low molecular weight agents (histamine and aminoacids). Mellitin and phospholipase are important components causing rhabdomyolysis following a toxic action on striated muscles and also act on red cell membrane and provoke hemolysis.[3] The elevated levels of enzymes CPK and aspartate-aminotransferase suggest the existence of rhabdomyolysis and hemolysis is suggested by anemia, unconjugated hyperbilirubinemia, reticulocytosis, increased serum LDH and hemoglobinuria.[3] Rhabdomyolysis and hemolysis can induce ARF, particularly in hypovolemic or acidotic individuals. It has been postulated that myoglobin and hemoglobin released from muscle or red blood cells cause ARF by toxic effects on tubule epithelial cells or by inducing intratubular cast formation. Hypovolemia or acidosis may contribute to pathogenesis of ARF in this setting by promoting intratubular cast formation. In addition, both hemoglobin and myoglobin are potent inhibitors of nitric oxide bioactivity and may trigger intrarenal vasoconstriction and ischemia in-patient with borderline renal hypoperfusion.[4] The most reported cases of ARF are as a result of mass stinging by Africanized honeybees. The components of venom in Africanized honeybees are similar to that of domesticated European honeybees.[1] Though the venom of Africanized honeybees is no more allergic or toxic than that of the European honeybees, the Africanized bees are unique in their aggressive behavior, characterized by massive attacks during which the victims are injected an important amount of venom and the mortality associated with Africanized honeybee attacks is primarily the result only of the number of the number of stings.[5] A number of about 500 stings have been considered necessary to cause death by direct toxicity,[3] but as few as 30-50 stings have proved fatal in child.[3] Our patient had about 200 stings and survived with complete renal recovery. The primary therapeutic goal is to prevent the factors that cause ARF, i.e. volume depletion, tubular obstruction, aciduria and free radical release. Patients are administered saline for intravascular volume expansion and sodium bicarbonate for urine alkalization (to urine pH level above 7). The ideal fluid regimen for patients with rhabdomyolysis consists of half isotonic saline (0.45%, or 77 mmol/L sodium), to which 75 mmol/L of sodium bicarbonate is added. Once overt renal failure has developed, the only reliable therapeutic modality is extracorporeal blood purification.[4] The treatment of severe ARF following Africanized bee stings with repeated hemodialysis, hemofiltration, or peritoneal dialysis has been described.[2],[3] Exchange transfusion or plasmaphresis has been found useful because it acts through a direct effect of reduction of the massive circulating venom or removal of the circulating mediators of inflammation caused by the venom itself.[3],[6] Taking into account the potentially lethal risks of plasmapheresis, this should be reserved for the treatment of life-threatening multisystem organ failure due to stings of members of the order Hymenoptera (honeybee, bumblebee, wasp, hornet, yellow jacket).[6] In conclusion, acute renal failure after bee stings is probably due to pigment nephropathy associated with hypovolemia. Early recognition of this syndrome is crucial to the successful management of these patients. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06030f1.jpg] |
| |||||||||

{kind=link}