 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
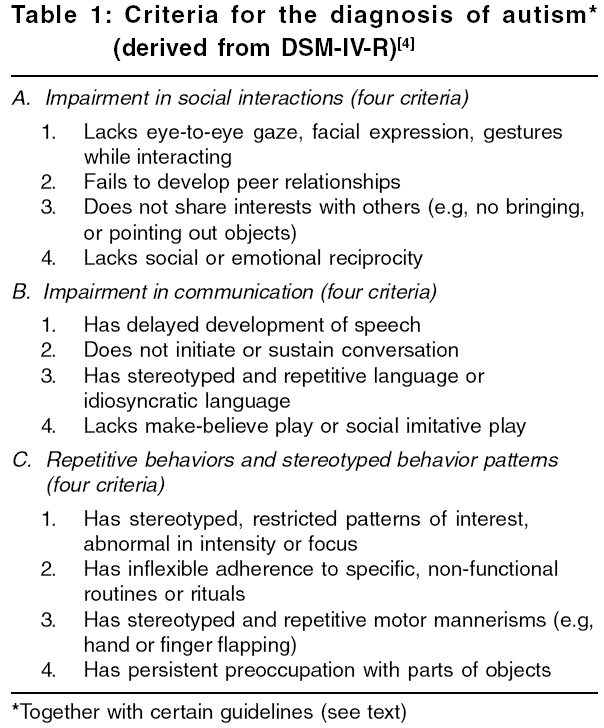
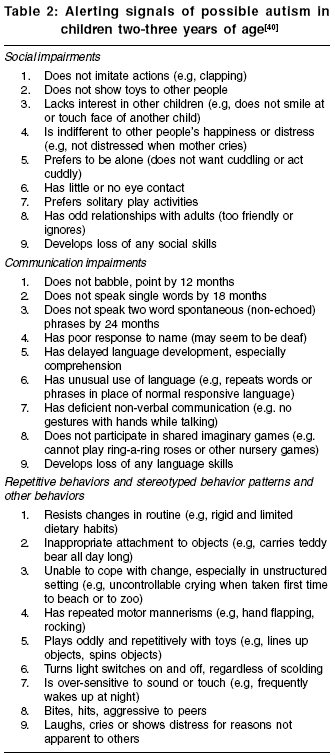
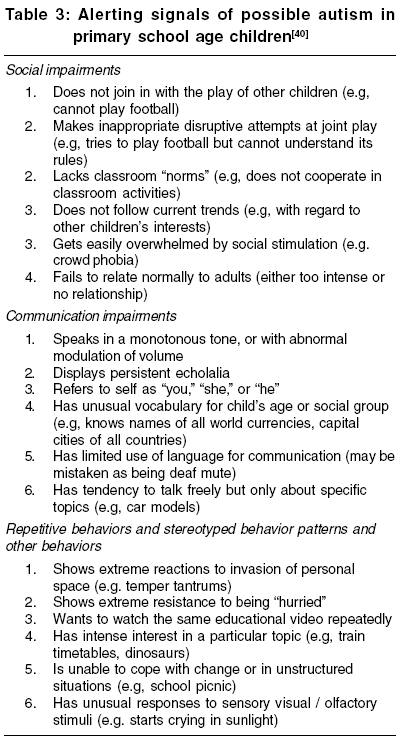
Indian Journal of Medical Sciences, Vol. 60, No. 5, May, 2006, pp. 205-215 Practitioners section Autism: A review for family physicians Karande Sunil Developmental Clinic, Division of Pediatric Neurology, Department of Pediatrics, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai - 400 022, India Correspondence Address:Sunil Karande, Developmental Clinic, Division of Pediatric Neurology, Department of Pediatrics, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai - 400 022, India. E-mail: karandesunil@yahoo.com Code Number: ms06031 Abstract Autism is a complex neurodevelopmental disorder characterized by qualitative impairments in social interaction and communication, with restricted, repetitive, stereotyped patterns of behavior, interests and activities. These behaviors manifest along a wide spectrum and commence before 36 months of age. Diagnosis of autism is made by ascertaining whether the child's specific behaviors meet the Diagnostic and Statistical Manual of Mental Disorders-IV-Revised criteria. Its etiology is still unclear but recent studies suggest that genetics plays a major role in conferring susceptibility. Recent neuroimaging research studies indicate that autism may be caused by atypical functioning in the central nervous system, particularly in the limbic system: amygdala and hippocampus. In a third of autistic children, loss of language and/or social skills occurs during the second year of life, usually between 15 and 21 months of age. Comorbidity with mental retardation, epilepsy, disruptive behaviors and learning difficulty is not uncommon. Although there is currently no known cure for autism there is evidence to suggest that early intervention therapy can improve functioning of autistic children. Judicious use of psychotropic drugs is necessary to manage associated aggression, hyperactivity, self-mutilation, temper tantrums; but drugs are not a substitute for behavioral and educational interventions. The family physician can play an important role in detecting autism early, coordinating its assessment and treatment, counseling the parents and classroom teacher, and monitoring the child's progress on a long term basis.Keywords: Autistic disorder, family physicians, primary care. Introduction Autism is not a single disorder but a name (derived from Greek ′autos′, meaning ′self′) given to a behavioural phenotype. Leo Kanner, a child psychiatrist, in 1943 first published a report describing 11 children with ′disturbances of affective contact′ and coined the term ′autism′ to describe the ′extreme aloneness′that he saw as its characteristic trait.[1] Kanner noted that these children demonstrated a profound lack of social engagement, failed to use language to communicate and had an obsessive need for sameness; and proposed that these problems were due to difficulties in the parent-child relationship.[1] Until the mid 1980′s, autism was wrongly viewed as a psychiatric disorder caused by parents who did not adequately love their children.[2] Since the late 1980′s, autism has been rightly recognized to be a ′neurodevelopmental disorder′; a behavioral symptom constellation due to underlying disorder of brain development.[2] The aim of this review article is to address the current issues concerning autism that are particularly relevant to the family physician. Diagnosis of Autism Family physicians should initiate an evaluation for autism when a child presents with qualitative impairment in social interactions, qualitative impairment in communication and/or with restricted, repetitive and stereotyped patterns of behavior, interests and activities.[3] Autistic symptoms occur along a wide spectrum.[3] Sensory hyposensitivities or hypersensitivities to the environment are often noted.[3] The diagnosis of autism is based on clinical findings and is made by ascertaining whether the child′s specific behaviors meet the DSM-IV-R criteria [Table - 1].[4] A child meets the diagnostic criteria for autism: (a) by documentation of at least six of the 12 behaviors described in the three domains [Table - 1], with at least two from the impairment in social interactions domain and one each from the impairment in communication and the repetitive and stereotyped behavior patterns domains; and (b) the onset is before 36 months of age.[4] Family physicians should make the diagnosis by focusing on the developmental story and systematically inquiring for core behaviors directly from the parents. The child should be observed in several settings as autism is a developmental disorder that unfolds over time.[5] The particular pattern of symptoms that presents in a two-year-old with autism may differ from that seen at the more prototypic age of four or five years.[5] In particular, overt repetitive and stereotyped behaviors may be less notable, although when these are seen alongside the social and communicative impairments they are highly indicative of autism.[5] Also, symptoms may vary in the same autistic child and change over time.[5] Prevalence of Autism A recent meta-analysis of 37 prevalence studies of autism reported from USA, UK, European countries and Japan has estimated that the prevalence of autism is 7.1 per 10,000 in individuals under 18 years of age.[6] Overall; boys are affected more often than girls and the average male: female ratio is 3.8:1.[7] In recent times in the USA and UK, population studies had suggested that the prevalence of autism has increased two to three times over the last three decades.[8],[9],[10] However detailed analysis of epidemiological data has revealed that the past rates underestimated true prevalence; and the current higher prevalence rates most probably reflect improved identification of autism rather than a secular increase in its incidence.[11],[12],[13],[14],[15] There is no data available from India of prevalence rates of autism in the general population. However, authors of recent case series reports of 16 and 62 autistic children from tertiary hospitals in Chandigarh and New Delhi, respectively, have stated that autism is not uncommon in India.[16],[17] Its diagnosis is frequently missed as there is tremendous lack of awareness and knowledge about the disorder among health professionals.[16],[17] What Causes Autism? There is no one single unified theory that explains the etiology of autism. Structural MRI brain studies have detected, though not consistently, increased volume of the total brain and abnormalities in the cerebellum, frontal lobe and limbic system (amygdala and hippocampus) in young children with autism.[18],[19] Recent functional brain imaging studies, such as positron emission tomography, single photon emission computed tomography and functional MRI studies indicate that autism may be caused by atypical functioning in the temporal lobes (where the amygdala are present medially) and an abnormal interaction between frontal and parietal brain areas.[20],[21] It has been postulated that early developmental failure in autism involving the amygdala has a cascading influence on the development of cortical areas, specifically the fusiform "face area" of the ventral temporal lobe. Development of face perception and social cognitive skills are supported by the amygdala-fusiform system and deficits in this network are instrumental in causing autism.[21] Pharmacological studies have implicated serotonergic dysregulation in the pathophysiology of the disorder as more than 30% of autistic children have elevated levels of serotonin in their platelets.[22] It has been postulated that at early stages of development, when the blood-brain barrier is not yet fully formed, the high levels of serotonin in the blood enter the brain of a developing fetus and cause loss of serotonin terminals. This results in damaged neurocircuitry which persists throughout subsequent development and eventually the symptoms of autism appear.[23] Family studies have provided strong evidence that genetics plays a major role in conferring susceptibility to autism.[24],[25],[26] Twin studies have reported 60% concordance for autism in monozygotic twins versus 0% in dizygotic twins.[24] The recurrence rate in siblings of affected children is approximately 2 to 8%, much higher than the prevalence rate in the general population.[25],[26] Recent research suggests that more than ten genes contribute to the underlying genetic risk of developing autism.[25],[26] It has been recently documented that close relatives of children with autism, who themselves do not meet criteria of autism, can have autism-related symptoms, viz. milder social and communication deficits and stereotyped behaviors.[27] In the last few years sensational media reports have blamed both the MMR vaccine and thimerosal (a preservative in multi-dose vaccine vials) for causing autism. However, epidemiological studies and related evidence do not support a causal link between MMR vaccination and thimerosal with autism.[28],[29] Comorbid Conditions Family physicians should be aware that almost 75% of children with autism have associated mental retardation.[30] Estimates for the prevalence of epilepsy in autistic children range from 7 to 14%, whereas those for the accumulative prevalence in adulthood range from 20 to 35%.[31],[32] Seizure onset peaks in early childhood and again in adolescence.[31],[32] All patterns of seizures are seen in children with autism.[31],[32] In addition to core symptoms, children with autism frequently have serious behavioral disturbances, such as self-injurious behavior, aggression, hyperactivity and temper tantrums in response to routine environmental demands.[33] In a small proportion, not exceeding 10%, autism occurs in conjunction with known medical disorders, prime examples being tuberous sclerosis, fragile X syndrome, phenylketonuria and congenital rubella syndrome.[7],[34] In approximately 25-30% of autistic children developmental regression occurs during the second year of life, usually between 15 and 21 months of age.[35],[36] This involves loss of word use accompanied by social withdrawal, loss of eye contact and play interests and sometimes increased irritability, change of sleep and eating habits.[35],[36] However, in many such cases, a careful history reveals that development of social communication was subtly abnormal before the onset of regression and the lost words may not have been used communicatively.[36] Even non-retarded autistic children may face a lot of scholastic problems in regular schools as their core features, which do not change qualitatively, impair learning.[37],[38] They often demonstrate distress and oppositionality when exposed to requests to complete academic tasks.[37],[38] Chronic learning difficulties can eventually lead to severe emotional distress, anxiety and even depression.[37],[38] How Early Can Autism Be Identified? Family physicians have an important role in early identification of children with autism. It is well recognized that the presence of a child with autism results in increased levels of parental stress and likelihood of disturbances to family and marital functioning. Careful attention to parents′concerns and specific inquiry into and observation of how children interact, communicate and play will help ensure that autism is detected early.[5] In the first year of life there are usually no clear discriminating features, but parental concerns should be elicited.[5] Interestingly, a detailed analysis of home videos taken by parents at around the first birthday of 11 children, who were later diagnosed to be autistic, has shown that these children already displayed four autistic behaviors viz. not pointing, not showing objects, not looking at others and failing to orient to name being called.[39] Abnormally accelerated rate of growth in head size between six to 14 months of age may serve as an early warning signal of risk for autism.[40] Studies have shown that autism can be reliably diagnosed at between two and three years of age.[41],[42] More severely affected children (in terms of both intellectual capacity and social communication) usually present in the preschool years (under five years) with language delay.[30] Asperger syndrome (AS) is a subgroup on the autistic spectrum.[30],[43] Children with AS share many of the same features as are seen in autism, but with no history of language delay and have an intellectual ability within the average or above average range. Children with AS have difficulty with social use of language and their social skill deficits make it difficult for them to make and maintain friendships.[30],[43] Children with AS tend to get diagnosed at a relatively older age on exposure to the greater social demands of the primary school environment.[30],[43] The following features should alert family physicians to the possibility of autism in children two-three years of age and in primary school age children [Table - 2][Table - 3].[44] The usefulness of screening instruments in detecting autism in the community in terms of sensitivity and specificity is still being debated.[5],[45],[46],[47] One such test, the ′Checklist for Autism in Toddlers′, was used to screen a total population of 16,235 children at the age of 18 months for autism.[46] The specificity of the test was high (97%), but sensitivity was too low (35%) to allow recommendation for use as a screening test.[46] Importance of early identification of autism There is emerging evidence that intervention therapy when initiated at an early age can improve outcome in children with autism.[48],[49] In addition, there is a need to give information regarding recurrence risks to parents who are planning another child.[50]Management of Autism A multidisciplinary team of professionals trained and specialized in autism is necessary.[48],[49] The team should include a developmental pediatrician, a child psychiatrist, an occupational (behavioral) therapist, a speech therapist, a psychologist, a specialist teacher and a social worker.[48],[49]
Initial assessment
Early intensive behavioral and educational intervention therapy As every autistic child is unique the interventions are highly individualized to target his/her specific deficits viz. deficits in imitation, attention, motivation, compliance and initiation of interaction. Skills are taught in small steps, mastered and then generalized. Individualized one-to-one therapy is provided in a distraction-free structured environment by behavioural therapists under supervision of a developmental pediatrician.[48],[49],[52] Only positive reinforcement is used to teach the child.[48],[49],[52] Parents are trained to generalize the skills learnt by their child in the home environment. Early intervention therapy not only reduces disruptive behaviors such as, aggression, hyperactivity and temper tantrums which impair learning but also prevents their development.[48],[49] The outcomes for children with autism are variable, reflecting the influence of comorbidities, such as intellectual handicap and mental health, as well as family functioning.[48],[49] Non-retarded autistic children who continue to experience difficulties in regular schools may need to attend special schools to continue their education.[37],[38]
Judicious use of psychotropic medications Management of Associated Epilepsy Symptomatic epilepsy needs to be treated and appropriate medication is prescribed depending on the seizure type.[58] However, care should be taken to avoid antiepileptic drugs such as phenobarbitone and phenytoin which are known to cause hyperactivity and impair cognition.[58]Important Role of Family Physician Every family physician can facilitate early detection of autism by specifically asking the parents during a consultation whether their toddler has an absence or delay of speech development, lacks normal interest in others or has regression of early speech and sociability.[5],[30] The family physician can play a crucial role in coordinating the assessment and treatment (convincing parents of the importance of intervention therapy, prescribing ongoing medication once the patient is stabilized; and ensuring compliance) of autism.[5],[30] Parents must be given information about appropriate schools and community-based support systems such as ′Action for Autism′(web site, http://www.autism-india.org).[30] The family physician can play an important role in counseling the parents and classroom teacher; and monitoring the child′s medical, social and academic progress on a long term basis.[5],[30] Parents of a child with autism may consult their family physician about the utility of unconventional therapies such as intravenous infusions of secretin, combined vitamin B6-magnesium treatment, casein and gluten free diets, sensory integration therapy, traditional occupational therapy, auditory integration therapy and music therapy to treat their child′s disorder. There is either insufficient evidence to support their use, or they have clearly proved to be ineffective when subjected to double-blind controlled clinical trials.[59],[60],[61],[62],[63] These unconventional therapies waste money and the child′s valuable ′early intervention therapy′ time; and therefore may adversely affect the child′s outcome.[30] The family physician can help parents become better-informed consumers. To conclude, every family physician can play a crucial role in helping a child with autism have a better outcome. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06031t2.jpg] [ms06031t1.jpg] [ms06031t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}