 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
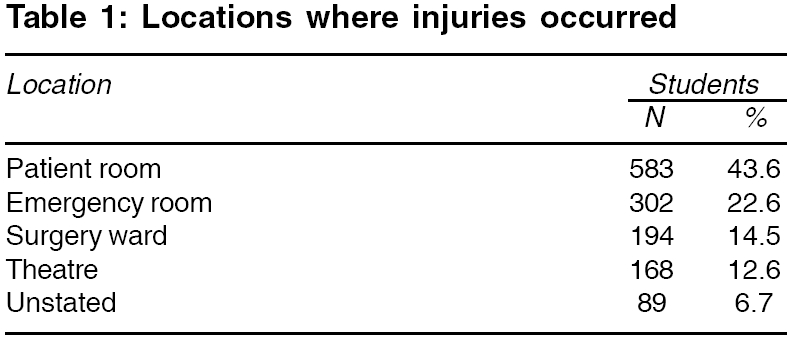
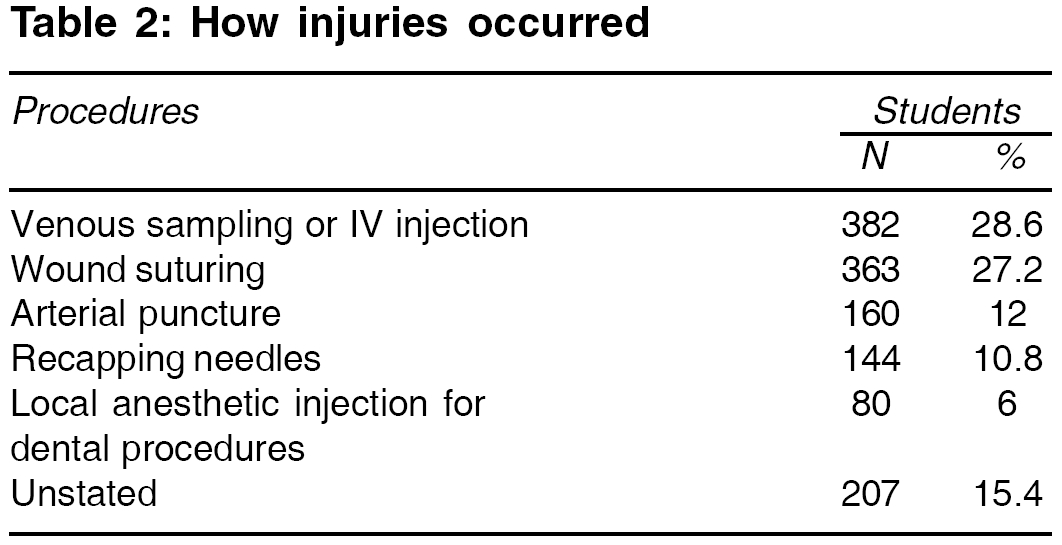
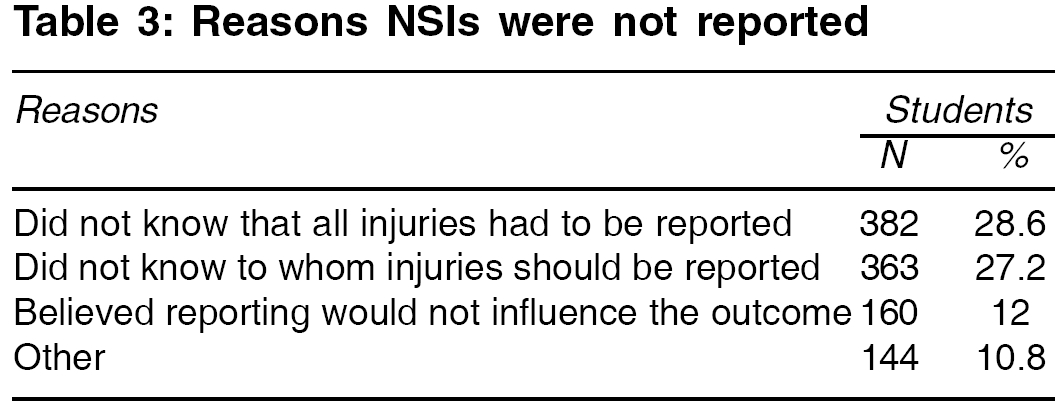
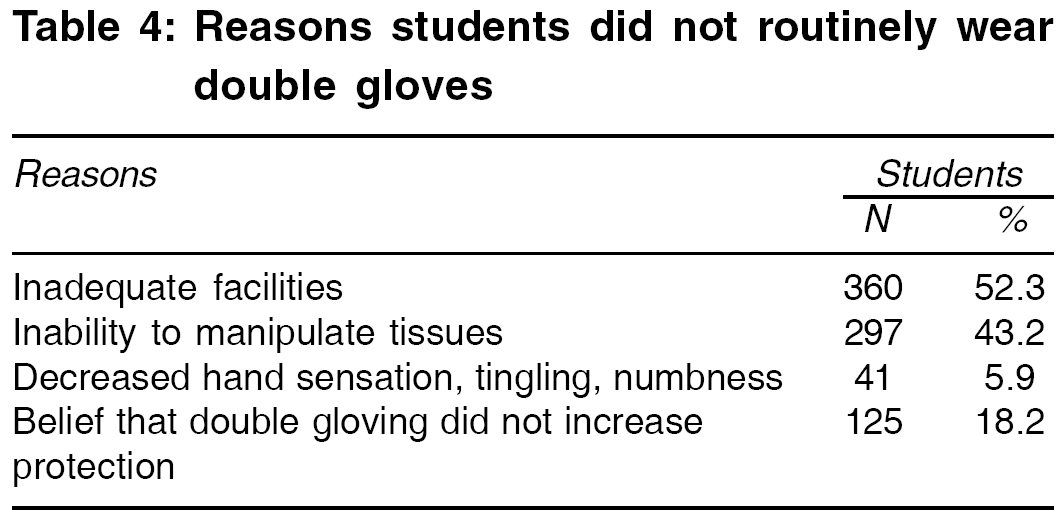
Indian Journal of Medical Sciences, Vol. 60, No. 6, June, 2006, pp. 227-232 ORIGINAL CONTRIBUTIONS THE PREVALENCE OF NEEDLE STICK INJURIES IN MEDICAL, DENTAL, NURSING AND MIDWIFERY STUDENTS AT THE UNIVERSITY TEACHING HOSPITALS OF SHIRAZ, IRAN Askarian Mehrdad, Malekmakan Leila Department of Community Medicine, Shiraz University of Medical Sciences, Shiraz Code Number: ms06032 Abstract BACKGROUND: Medical, dental, nursing and midwifery students are at high risk for occupational exposure to blood-borne pathogens (BBPs) via sharp injuries such as needle stick injuries (NSIs). Keywords: Blood-borne pathogen, dental student, medical student, midwifery student, needle stick injury, nursing student. One of the serious problems of medical and paramedical students is the risk of occupational exposure, via sharp injuries, to blood-borne pathogens (BBPs) such as Hepatitis B (HBV), Hepatitis C (HCV) and human immunodeficiency virus (HIV).[1],[2],[3],[4],[5],[6] Thirty percent of needle stick injuries (NSIs) are not reported in the United States.[7] The risk of pathogen transmission from infected persons to nonimmune persons through an injury with a sharp object has been estimated to be between 6 and 30% for HBV, between 5 and 10% for HCV and 0.3% for HIV.[7],[8] Effectiveness of administration of post-exposure prophylaxis varies from 75 to more than 90% to prevent HBV infection. Post-exposure prophylaxis for HIV has also been shown to lower the risk of infection after sharp injuries. However, there is no known way of preventing HCV acquisition following NSI.[7],[9] The purpose of this study was to calculate the frequency and the circumstance of NSI among a group of health care students as well as their knowledge, attitude and practices regarding the use of protective strategies against exposure to blood-borne pathogens (standard isolation precautions, double gloving and post-exposure prophylaxis).[10] Materials and Methods All 1,299 medical, dental, nursing and midwifery students during clinical training at Shiraz University of Medical Sciences were eligible to participate in a survey conducted by an anonymous self-administered questionnaire in 2004 that asked them about NSIs during their clinical training undergraduate years after having oral informed consents. The proposal, including ethical views, was approved by the University′s Vice Chancellor of Research. The survey tool was a questionnaire that was pre-tested on a random sample of 55 participants to ensure practicability, validity and interpretation of responses. The reliability of the questionnaire was assessed using Cronbach′s alpha (0.812). Statistical analysis Results The survey was completed by 688 (53%) students of whom, 343 (57.2%) were medical, 208 (47.8%) were nursing and midwifery and 137 (51.9%) were dental students, consisting of 386 female and 302 male students. Since entering their clinical year, 71.1% (489/688) experienced a total of 1,336 NSIs, giving a ratio of 1:1.9 NSIs sustained by students in their undergraduate clinical school over, on an average, a-12 month period (maximum 17 months). For the students who reported that they had sustained an NSI, 27.8% (136/489) had one, 18.8% (92/489) two, 13.5% (66/489) three and 39.9% (195/489) more than three NSIs. The majority ( P < 0.043, df=3,485, CI=4.308-2.708) of all NSIs were sustained in patients′rooms and occurred most frequently during venous sampling or intravenous (IV) injections [Table - 1][Table - 2]. For the last injury recalled, 74.6% (365/489) involved students injuring themselves. Overall, 82% (401/489) of all NSIs went unreported, most of which were because the injured student did not know about the reporting mechanism [Table - 3]. The reasons given by students who did not routinely wear double gloves were inadequate facilities and decreased ability to manipulate tissues [Table - 4]. Few (35.6%-245/688) students reported that they always used sharp containers to dispose needles and 11.6% (80/688) practiced recapping rarely or never. Eye protection in the operating and emergency rooms was not used routinely by the majority (97.5%) of medical and nursing students. 52.5% of the dental students used eye protection routinely. HBV vaccination coverage was 86.2% (594/688). Of all NSIs, 2.5% (34/1336) of needles had been used on patients with HBV infection, 1.6% (22/1336) with HCV infection and 0.4% (6/1336) with HIV/AIDS. Most students (58.1%, 400/688) were either extremely or very concerned about the possibility of contracting HBV infection. The students rated patient risk factors on a five-point scale, ranging from extreme to no concern. Most had extreme concern for the acquisition of AIDS (94.5%-651/688), HBeAg positive HBV infection (94.5%-651/688) and injecting drug users (88.5%-609/688). Discussion This is the first survey of needle stick injuries (NSIs) in Shiraz, Iran. NSIs are one of the hidden problems in health care workers.[2],[3],[4] In our study, 71.1% (489/688) of the students reported at least one NSI, most of which occurred in patient rooms during venous sampling or intravenous injections. Many (30%) of the medical students in Washington had sustained at least one NSI and these most commonly (72.1%) occurred in the operating room.[2] Most students (61.9%) in Taiwan had an NSI and the majority (70.1%) of these NSIs occurred in patient rooms.[3] In Iran 31.7% of 203 anesthesiology personnel had at least one NSI.[8] In other studies, it has been shown that lack of experience in many procedures, insufficient training, work overload and fatigue leads to occupational sharp injuries.[10],[11],[12] In this study, 82% (401/489) of the students did not report these NSIs. The most common reason for under-reporting was the personnel′s lack of knowledge that all injuries had to be reported [Table - 3]. Other reasons are based on a background of insufficient knowledge or poor practices. The observed high level of under-reporting suggests that students need education on prevention, especially focusing on the importance of reporting all NSIs and the possibilities of prophylaxis after exposure to BBP.[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13] Our study showed that 87.8% (604/688) of the students reported receiving information about Universal Precautions (UP) and BBP exposure. This is lower than the figure arrived at in the study by Patterson et al which evaluated NSIs among medical students and found that 98% of them reported receiving information about these topics.[2] These data show that the students need to be provided structured education in UP for the improvement of occupational safety.[14],[15],[16],[17] In our study, only 86.2% (594/688) of the students reported having received three doses of vaccine and most students (96.2%) reported gloving during wound suturing. Meaner et al reported that 50% of medical students in Strasbourg did not use gloves.[18] In our study, 11.6% (80/688) of the students practiced recapping ′rarely to never′ and 35.6% (245/688) of them always discarded needles in a sharp container. 58.1% of the students in this survey were extremely or very concerned about BBPs. That is similar to the study of Bilsk et al that reported that the most common cause of injuries from needles in nurses was improper handling of syringes and needles after injections (removing a needle from a syringe or placing the needle in a full container for medical waste).[19] 87% of the medical students in Washington were moderately to extremely concerned about BBP.[2] Our study revealed that the majority of students were either extremely concerned or very concerned about the possibility of contracting HBV infection (58.1%-400/688). 30.9% (213/688) of students also stated that their concerns had influenced their decision on choosing a specialty residency. Also, this concern and attitude about BBP transmission can influence their practice. However, it can be speculated that extended knowledge on this issue and professional counseling after exposure might lead to a changing attitude. Recently, a study conducted at an Australian hospital demonstrated that NSI events represent an important workplace issue for nurses.[20] The results of this study show that the way of educating about NSIs has to be changed so that health care workers realize the importance of occupational exposure UP and other protection strategies for blood-borne infections. We need further evaluation of the effectiveness of improved education in the workplace. We recommend a surveillance system and a center for managing injured persons in each and every ward of hospitals to be set up as well as following up injured health care workers as part of a local research or ongoing audit project. Success of educational and other interventions as well as risks for different specialties or professional groups also need to be assessed in this way. In conclusion, these students are at high risk for NSIs and BBPs exposure and we recommend that they need a targeted education about protection strategies for blood-borne infection. Acknowledgement This study was funded by the Deputy for Research at the Shiraz University of Medical Sciences (grant no. 82-1961).References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06032t1.jpg] [ms06032t4.jpg] [ms06032t3.jpg] [ms06032t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}