 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 60, No. 7, July, 2006, pp. 271-276 ORIGINAL CONTRIBUTIONS TOBACCO USE AND CARDIOVASCULAR DISEASE: A KNOWLEDGE, ATTITUDE AND PRACTICE STUDY IN RURAL KERALA Tiwari Rajnarayan, Deb Pankaj, Debbarma Aghore, Chaudhuri Rupali, Chakraborty Amita, Lepcha Mickyla, Chakraborti Gita National Institute of Occupational Health, Meghani
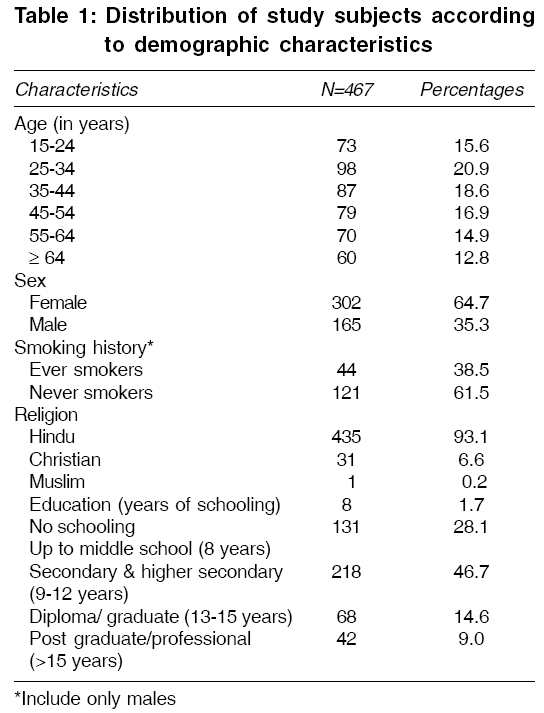
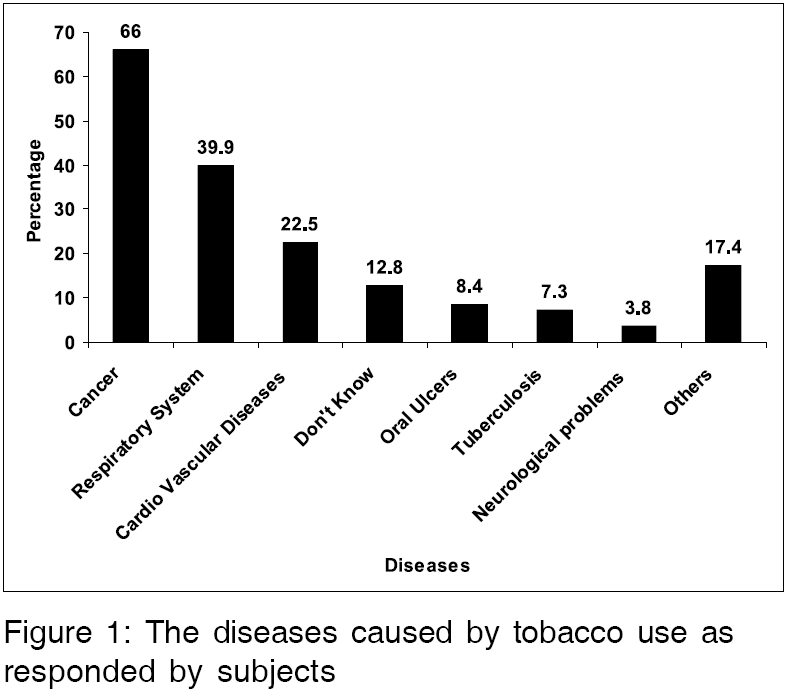
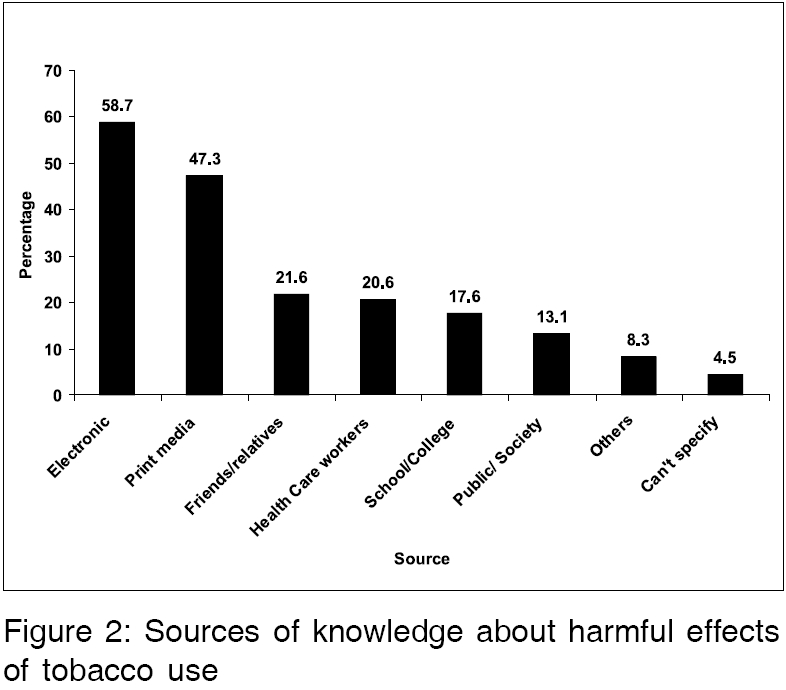
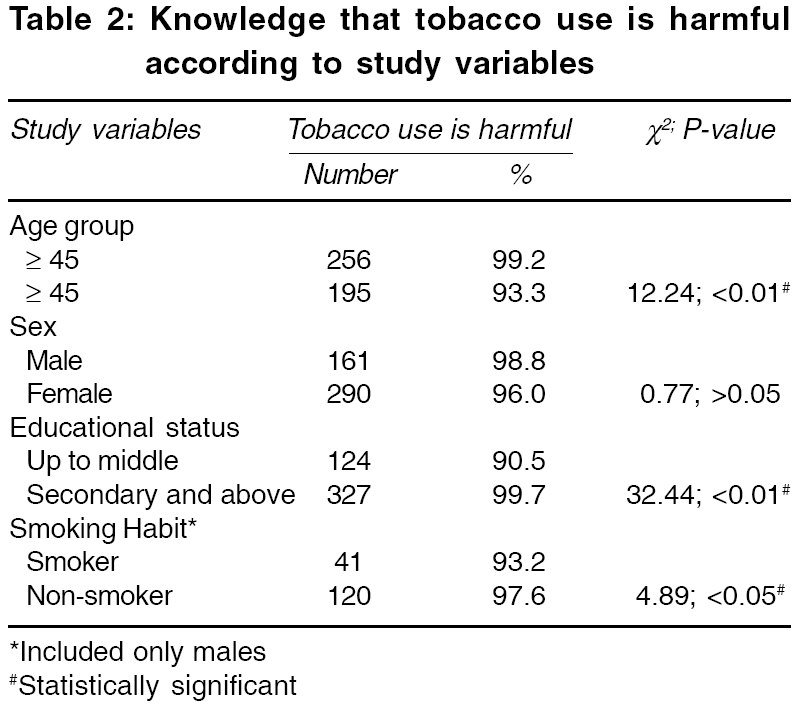
Nagar, Ahmedabad Code Number: ms06039 Abstract BACKGROUND: Tobacco consumption, either in smokeless form or as smoking, is reported to be responsible for major non-communicable diseases, namely, cardiovascular diseases, chronic obstructive pulmonary diseases and cancers. Whatsoever control strategy is being used, the community participation is of utmost importance, which will depend largely on the level of the knowledge in the community.AIM: To assess the knowledge and attitude of a rural community towards the harmful effects of tobacco use. SETTING AND DESIGN : Venganoor Gram Panchayat of Thiruvananthapuram district of Kerala; cross-sectional study. MATERIALS AND METHODS: Interview schedule was used to collect the information on pre-designed and pre-tested proforma. The information recorded, included the demographic characteristics and socio-economic characteristics. The awareness regarding tobacco use and the attitude towards its non-usage was done, by putting forward, open and closed-ended questions. STATISTICAL ANALYSIS: Percentages and proportions; t-test; chi-square test. RESULTS: The present study included 302 (64.7%) females and 165 (35.3%) males. Among the males, 44 (38.5%) were ever smokers. Though 451 (96.6%) of the subjects knew that tobacco use is harmful for health, only 101 (22.5%) of the subjects knew that it causes cardiovascular diseases. Electronic and print media were the common source of such knowledge being reported by 265 (58.7%) and 202 (44.7%) subjects, respectively. CONCLUSIONS: The subjects were aware about the harmful effects of tobacco use. However, more efforts are needed to make them aware about the role of tobacco smoking and chewing, in causing cardiac problems. Keywords: Attitudes, awareness, cardiac problems, health knowledge, humans, practice, rural Kerala, smoking/adverse effects, tobacco use Tobacco use is one of the major preventable causes of death and disability worldwide. The emergence of tobacco- related diseases are a burgeoning public health problem. According to recent WHO estimates, 4.9 million deaths annually, are attributed to tobacco.[1] This figure is expected to rise to 10 million in 2030, with 7 million of these deaths occurring in developing countries, mainly China and India.[2],[3] Currently, about one-fifth of all worldwide deaths attributed to tobacco, occur in India, where more than 800,000 people die and 12 million people become ill as a result of tobacco use each year.[3],[4],[5] With the current smoking pattern, about 500 million people who are alive today, will eventually be killed by tobacco use. More than half of these future deaths will occur among today′s children and teenagers.[5] Tobacco consumption, either in smokeless form or as smoking, is reported to be responsible for major non-communicable diseases namely, cardiovascular diseases, chronic obstructive pulmonary diseases and cancers.[6],[7],[8] Thus, most of the control strategies revolve around the control of tobacco use. Whatsoever strategy is being used the community participation, is of utmost importance for the programme to be successful. Though many studies have been carried out to know the harmful effects of tobacco,[9],[10],[11],[12] very few studies have been carried out regarding community awareness about the role of tobacco use in causing cardiovascular diseases. Thus, the present study has been carried out to assess the knowledge and attitude of a rural community towards tobacco use. MATERIALS AND METHODS The present cross- sectional study was carried out in one of the anganwadi areas of Venganoor Gram Panchayat, in the Thiruvananthapuram district of Kerala, during December 2004 to March 2005. This anganwadi area was randomly selected. This randomization included preparation of the list of Gram Panchayats in the Thiruvananthapuram district of Kerala. By lottery method, the Venganoor Gram Panchayat was selected. This was followed by preparation of a list of anganwadis in the Venganoor Gram Panchayat and again, by selection of the anganwadi by a lottery method. This randomly selected study area included 249 houses, of which 222 houses were included in the present study. The remaining houses could not be covered, because they were locked and nobody could be found in spite of repeated efforts. In the covered houses, there were 953 people, of which only 755 subjects were aged ≥ 15 years. In the present study, 467 subjects were included, thereby giving a total population coverage of 61.9%. After taking the informed consent from the subjects, an interview schedule was used to collect the information on pre-designed and pre-tested proforma. The information recorded, included the demographic characteristics and socio-economic characteristics. For the present study, all those who have smoked at least one cigarette or bidi in the last one-month period were considered as current smokers, while those who have left smoking since ≥ 1 year were considered as ex-smokers. For the analysis purpose, the current smokers and ex-smokers were categorized in the group of " ever smoker". The awareness regarding tobacco use and the attitude towards its non-usage was done by puttingforward, open and closed- ended questions. Questions such as the diseases caused by tobacco use and the sources for such knowledge were open- ended, while the questions to assess whether they had knowledge on the harmful effects of tobacco use and whether they would advise others to quit smoking, were close- ended. Statistical analysis was carried out using Epi Info version 3.3, included calculation of percentages and proportions and application of tests of significance such as chi-square test and t-test. RESULTS [Table - 1] describes the prevalence of different risk factors among study subjects. The present study included 302 (64.7%) females and 165 (35.3%) males. More females than males were included in the study, because it was a house-to-house survey carried out on weekdays, when most of the males go for work and only females stay at home. Though efforts were taken to include the left-over male subjects by carrying out the survey on Sundays and holidays, the number could not be increased. The greatest number of subjects (20.9%) was in the 25-34 year-old age group. The mean age of males was 43.5 ± 18.8 years, while that of females was 42.5 ± 16.3 years. The difference was found to be statistically non-significant (t=0.34, df=1, P =0.56). None of the females reported to have a smoking habit or history of the use of alcohol. Among the males, 44 (38.5%) were ever smokers. 218 (46.7%) study subjects had 9-12 years of schooling, while only 8 (1.7%) of the subjects had no schooling and were illiterate. This is substantiated by the fact that the literacy rate of Kerala is highest among all the states of India. The mean years of schooling for both males and females, was 10 years. Out of 467 subjects, 451 (96.6%) subjects accepted that the use of tobacco is harmful for health. [Figure - 1] depicts the health conditions caused by the use of tobacco, either in chewing or smoking form, as reported by the study subjects. When asked about the common diseases caused by the use of tobacco in any form, multiple responses were obtained. 298 (66%) subjects said that cancers were caused by tobacco use, while only 101 (22.5%) said that tobacco use results in cardiovascular diseases. 78 (17.4%) subjects reported unusual diseases like blood cancers, liver problems, mental health problems, etc. Others reported tuberculosis 33 (7.3%) oral ulcers 38 (8.4%) and CNS problems 17 (3.8%). 58 (12.8%) of the subjects mentioned that they know that tobacco use is harmful, but they could not tell about the diseases caused by it. [Figure - 2] shows the sources of knowledge about the harmful effects of tobacco use. Electronic and print media were the common sources of such knowledge being reported by 265 (58.7%) and 202 (47.3%) subjects, respectively. Only 93 (20.6%) subjects reported that health-care workers were a source of such knowledge. Other sources included friends and relatives 97 (21.6%), being told in schools/colleges 79 (17.6%) and knew from the discussions going on in public/society 59 (13.1%). 20 (4.5%) subjects could not specify the source from where they got this knowledge. [Table - 2] depicts the differences in knowledge in some of the study variables. The knowledge that tobacco use in any form is harmful to health, was more pronounced among younger subjects than older ones. This difference was found to be statistically significant (χ 2=12.24; df=1; P < 0.01). The knowledge was almost similar for both sexes. A significantly less number of those who had up to middle level education, knew about the harmfulness of the tobacco use, than those educated upto secondary level and above (χ 2=32.44; df=1; P < 0.01). More non-smokers than smokers had knowledge about the harm caused by tobacco use (χ 2=4.89; df=1; P < 0.05). When asked whether they advised others to quit smoking, only 323 (69.2%) gave an affirmative response and it was equally distributed among both sexes. However, females usually advise their husband or relatives, while males usually advise their friends. A significantly less number of smokers 21 (47.7%) was found to advise others to quit smoking, as compared to non-smokers 92 (76%). The difference was found to be statistically significant (χ 2=11.7, df=1, P =0.001). DISCUSSION The present study revealed that only 22.5% knew about the effects of tobacco in causing cardiac problems. Most of the subjects knew its harmfulness in causing cancer. This may be due to the active campaigning by the health care workers from the Regional Cancer Centre. Earlier studies among different groups have also reported similar findings.[13],[14] Electronic and print media were more common sources of such knowledge, as compared to health education provided by health care workers. This may be due to the easy accessibility of these two sources, as compared to health care workers. Schools and books, which were thought to be an important source for such information, constitute a small percentage. Gajalakshami[13] et al in their study, also found that only about half of the students reported that they have been taught about the harmful effects of tobacco use in school, during the year preceding the survey. Similarly, Sinha[15] et al reported that merely 3% students were taught in school about the harmful effects of tobacco. Age, level of education and smoking habits were found to be the factors associated with the knowledge about the harmfulness of tobacco use. Sarma[16] et al also reported that smokers continued to smoke despite being averse to smoking and disapproval of their habit by their family members. Less number of smokers was found to advise others to quit smoking, as compared to non-smokers. This may be because of the feeling among smokers, that others may be reluctant to listen to their advice regarding quitting smoking, when they themselves use tobacco. A similar finding was reported in an earlier study among doctors, which reported that patients were counseled about smoking hazards by smoking doctors and surgeons, who practised it significantly less often.[17] The limitations of the study include small sample size and low response rate. However, every effort was taken to contact the persons who were left out, in order to increase the response rate. However, only 60.8% of the subjects could be covered. Thus, to conclude, it can be stated that more efforts are needed to make the subjects aware about the role of tobacco in causing cardiovascular diseases. On the basis of the present study, it is recommended that health education programmes are required more often and these education programmes must also provide information about the harmfulness of tobacco use in causing cardiac problems, along with other hazards. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06039f1.jpg] [ms06039f2.jpg] [ms06039t2.jpg] [ms06039t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}