 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
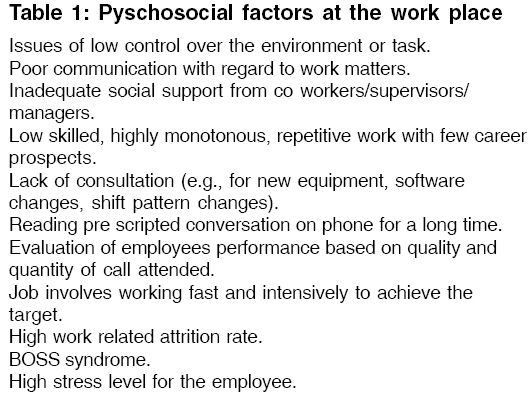
Indian Journal of Medical Sciences, Vol. 60, No. 7, July, 2006, pp. 300-307 Practitioners section WORKING CONDITIONS AND HEALTH AMONG EMPLOYEES AT INFORMATION TECHNOLOGY - ENABLED SERVICES: A REVIEW OF CURRENT EVIDENCE C. KESAVACHANDRAN, S. K. RASTOGI, MOHAN DAS, ASIF M. KHAN* Epidemiology Section, Industrial Toxicology Research Centre (ITRC), Council of Scientific and Industrial Research (Govt. of India), Lucknow, *Dept. of Biotechnology, National First Grade College, Bangalore University, Bangalore, India Code Number: ms06044 Abstract Workers in information technology (IT) - enabled services like business process outsourcing and call centers working with visual display units are reported to have various health and psycho social disorders. Evidence from previously published studies in peer- reviewed journals and internet sources were examined to explore health disorders and psycho-social problems among personnel employed in IT-based services, for a systematic review on the topic. In addition, authors executed a questionnaire- based pilot study. The available literature and the pilot study, both suggest health disorders and psychosocial problems among workers of Business Process Outsourcing. The details are discussed in the review.Keywords: Employees, health and psycho-social problems, humans, IT-enabled services, cumulative trauma disorders/etiology, Occupational diseases/etiology, user-computer interface For many information technology-enabled Services [ITES] operators, the work consists mainly of activities that use telephone and computer, with the objective of developing standardized and continuous actions of marketing or to manage communication with clients, public or government agencies. In spite of the growth of the number of centers of ITES, a modernization of processes and organizational planning in these new work environments, did not take place. The result was an increase of the turnover, absenteeism and occupational diseases.[1] Computer work has generated a new genre of occupational health problems, i.e., of computer-related problems. In India, the occupational health personnel is slowly awakening to this group of modern occupational diseases, which are slowly taking its roots among the information technology (IT) professionals. These problems if ignored, can prove debilitating and cause crippling injuries, forcing one to change one′s profession.[2],[3] A call center operator′s tasks involve the use of computer. Among computer operators, risk factors associated with work-related musculo-skeletal disorders, include the integration of biomechanical factors such as static muscular overload, repetitive motions, conditions related to the work station and work environment and issues related to the working organization, as well as those associated with the psychosocial aspects of work.[4] There is a growing need to study the health status among the employees at ITES, since the number of workers is rapidly growing and will touch 1.2 million in the next three years from a figure of 2,50,000 in March 2004, according to National Association of Software and Service Companies.[5] The stress factors, the working conditions and the ergonomic stature of the employees in this sector [Table - 1], is causing several psycho-social and health problems. It must be pointed out that there are not many studies that have directly addressed the health and psycho-social problems in ITES workers. Therefore, there is a need to have a comprehensive review article on the subject, in order to create awareness and mitigate the risk factors in the industry. This review treats the work organization, psychosocial well-being and health disorders of workers in ITES from the available literature, including the author′s study on the workers health in IT- enabled services. Working organization in ITES workers Ergonomic work analysis showed that the operator′s tasks included receiving the customer′s inquiry, seeking the correct information in the data system and communicating this information to the customer, as well as inputting information. Incoming calls were directed by a central computer to the next available operator. The operator had no control of the period of time, between calls. The system registered the time taken until the customer was connected, the duration of each call and developed the average amount of time per call for each operator, as well as the number of calls taken by each operator. Operators had to follow a pattern established by the enterprise of 90 to 140 calls per day and an average call time of two minutes. Operators could disconnect themselves from the system in order to take care of personal necessities, but the number of times they did so, the duration was registered. The daily working time was 6 hours, with one rest break for recovery, of 30min. Employees have to attend peak connections during Mondays and Fridays in a week, in the end of the month and immediately after a holiday.[1] The Health and Safety Executive (HSE) estimates that between 1-1.7% of the total United Kingdom workforce are employed in call centers, with a predicted rise of 2% in the next 3 yrs. The HSE estimates that there are between 900 and 1300 call centers in Great Britain, some of which are departments of large organizations such as banks and some of which just exist as telecommunication centers. HSE has recently suggested that "Call centers are a unique working environment", because of a combination of factors; electronic performance and monitoring and having to spend extended, intensive periods working with both a telephone and computer.[6],[7] The majority of data processors reported that they had to work fast and intensively. Low levels of job controls (i.e., how and when should they do their work, when they could take breaks) were also reported. Nearly half the data processors reported that they didn′t get help from colleagues or supervisors to complete the task, if time was limited.[8] Call center workers have to listen, watch and talk, all at same time, without a break. The odd timings and nature of work by sitting in a chair for 9 hours a day, reading pre-scripted conversations on the phone endlessly and often to irate customers from across the globe, make the job more stressful. The employee′s time is recorded, measured and automatically logged onto a computer for praise or censure, on a weekly basis. Evaluation of the performance of the operators is based on the average call time and number of calls attended and qualitative aspects related to the supervisor′s appraisal of the operator′s responses to the customer. The supervisor evaluates the calls taken by employee, using electronic monitors based on the company′s rules and procedures, the sales and the promotional campaigns and the courtesy and the quality of the service being delivered.[1] The performance monitoring also puts enormous stress on the employee.[9] Forty-seven percentage of female call operators stated that they answered more than 140 calls daily, 59% of them stated they had little work control, 69% indicated that fast pace was an issue and 47% stated that their work was a source of stress. Among the male operators, 8% stated that the number of daily calls handled exceeded 140, 23% stated they had little work control, fast pace was an issue for 15 and 15% also stated that work was a source of stress. The complexity of the tasks was a result of the diversity of customers attended and of the services and procedures requested. Twenty percent of data processors were dissatisfied with their jobs. Twenty- one percent were dissatisfied with the help/support from supervisors and 12% were dissatisfied with the help/support from colleagues.[8] The food habits and nutritional assessment conducted by Choudhary et al[10] among computer professionals, reveal skipping of break fast (36%), skipping of meals (28%), changed food habits (48%), vegetarian food habits (45%), consumption of alcohol of more than 150 ml/day (1%) and excess caffeine intake (18%).[10] Health and Pyscho-Social problems A recent study[5] conducted by VV Giri National Labour Institute, Noida, India, on a case study of call centers, found that women (between 20-30 years age group) constituted about 38 percent of the work force sampled. Shah et al[11] reported the mean age of 25.4 years among computer professionals in the study, while Suparna et al[12] had subjects with mean age of 29.86 years and Chaudhary et al[3] had subjects with mean age of 29 years. The males outnumbered females in the ratio of 7:3, in the studies conducted in India.[3] The studies done in India had predominantly male workers unlike most studies in western world, where female workers outnumber males. The profile of a typical woman in this sector was young, educated and unmarried, with an urban background. Call centers engage women for jobs such as attending credit card enquires or telemarketing campaigns. The study noted that the continued stress and strain at work lead to circumstances, where women find it difficult to carry on, especially during pregnancy and in situations of double burden of family and work. Eighty five percent of women in Business Process Outsourcing (BPOs) were found working on night shifts. A very high attrition rate was found among women. The major reasons cited for quitting the job by employees, were inconvenience of shifts, increased stress, and lack of career prospects. The majority among the female work force in BPOs was found to be predominantly unmarried, those without too many household obligations. Those who were above 30 years and married, were found to be living under special circumstances - they were divorcees, mothers of grown up children or married to call center employees. This suggests that work in call centers is equally or more women-unfriendly, compared to traditional manufacturing sector jobs.[5] The call center ranked high for attrition due to health reasons. Sleeping disorders were observed among 83% compared to the industry average of 39.5% and voice-loss among 8.5% as against 3.9%. Other health problems are ear problems (8.5%), digestive disorders (14.9%) and eye- sight problems (10.6%).[9] An earlier study[13] showed that personal noise exposure of call center operators is unlikely to exceed the 85 db level. The risk of hearing damage is therefore low. The burn out stress syndrome (BOSS) is commonly observed among young people working in call centers. The symptoms of this syndrome include chronic fatigue, insomnia and complete alteration of the 24 hour biological rhythm of the body, leading to sickness absenteeism.[14] The authors conducted a pilot study based on a postal questionnaire survey during 2005, on thirty computer professional workers working in different Information Technology- enabled services (ITES) for more than 2 years, with more than 4 hour′s computer use in different operations. Workers were in the age group of 22 to 30 years (Mean ± SD 28 ± 3.18 years), having mean body height in cms (172.05 ± 7.84) and body weight in kg (70.68 ± 11.76). The preliminary study revealed an overall morbidity of 70%. Predominant morbidity of musculo skeletal disorders (MSD) were observed among 56% computer professionals. Among the MSD, the shoulder (20%) arm pain while using mouse (5%), pain in fingers (7%), wrist pain (6%) and lower back pain (18%) constitutes the main findings, while visual problems were detected in 8% cases and 17% suffered from headaches. No such health complaints were recorded in the controls belonging to the similar age and socio economic group, who were never worked in ITES. Musculoskeletal pain and visual discomfort are the main health problems reported by computer workers[15],[16] and the major contributors to lost workdays.[17] Among the computer operators, risk factors associated with musculo-skeletal disorders include the integration of biomechanical factors such as static muscular overload, repetitive motions, conditions related to the work station and work environment related to the working organization, as well as those associated with the psychosocial aspects of work. Eighty six percent of data processing workers reported musculo-skeletal pain and discomfort. The main body areas of concern for data processors were the neck, lower and upper back, wrists/hands, shoulders and left elbow pain/discomfort. Eighty one percent of data- processing staff attributed their pain and discomfort to work due to poor seating (49%), constant keying (24%), sitting in the same position for hours (23%) and computer set up (12%).[8] Electromyography studies (EMG) of extensors and flexors of the forearm was conducted on Group I (executives whose job included trouble-shooting electronic circuits using computer based software), Group II (included executives whose job involved designing of software, verification of programs and actual loading of the program for performance evaluation), Group III (executives in the electronic computer- aided design), and Group IV (middle- aged personnel who would carry out their work of designing and processing of the electronic data on the computer). The executives showed fatigue at the end of the work shift, in a significant percentage (Group I-17, Group II-40, Group III-16 and Group IV-27%) of the computer users. Low back ache (Group I-61%, Group II-53%, Group III-33% and Group IV-45%), straight spine syndrome (Group I-30%, Group II-23%, Group III-33%, Group IV-27%) and carpal tunnel syndrome (Group I-9%, Group II-17%, Group III-16%,Group IV-18%) were present in a significant percentage of the population, indicating that work- related musculo- skeletal disorders (WRMD) are the second most prevalent disorders in the IT professionals.[18] Similarly 86% female and 68% male call center staff reported musculo -skeletal problems, especially pain in neck and shoulder regions.[19] Physical workplace factors (e.g., prolonged static muscle load, workstation factors) have been identified as risk factors for musculo -skeletal diseases (MSD).[8],[20],[21],[22] In the computing environment, incorrect computer workstation set up,[23] prolonged work in fixed or awkward positions,[24],[25],[26] seated and static work and overuse[27] have been identified as MSD risk factors. A relationship between upper extremity pain and duration of keyboard use, has also been documented.[28] In addition, relationships exist between psychosocial factors (e.g., social support from colleagues/supervisors) and musculo - skeletal pain.[28],[29],[30],[31],[32] Increased risk of fore arm pain was associated with use of a mouse device for more than 30 hours per week and with keyboard use more than 15 hours per week. High job demands and time pressure at baseline were risk factors for onset of these musculo-skeletal problems among women. Kryger et al[33] had shown two- fold increased risk of developing forearm pain. Intensive use of a mouse device and to a lesser extent keyboard usage, were the main risk factors for forearm pain. In a prospective population based study, psychological distress and other somatic symptoms were found to correlate with onset of forearm pain, in addition to work- related mechanical factors (repetitive movement of arms) and psycho social factors (lack of support from supervisors and colleagues).[34] Serum creatinine kinase concentration were normal in 96% of the IT professionals, showing that there was no muscular damage.[18] A health survey conducted by Choudhary et al[10] on professionals working in software development, showed neck and shoulder problems in 31%, wrist and hand pain in 15%, tiredness at the end of the day in 26% and exhaustion in 12%. Sobratty and Korumtolle[35] showed a high prevalence of visual problems (59.5%) among computer professionals. Monitor height and glaze angle also affect the eyes and lower monitor height are likely to reduce eye discomforts.[36] The study conducted on computer professionals by Parekh et al ,[37] showed that the symptoms increased with duration of span of computer use and with use of improper furniture. The symptoms were also more in spectacle-wearers, compared to non-spectacle users. The visual strain is also related to musculo-skeletal complaints and work stress.[17] The visual problems were seen in 76% and musculo- skeletal problems in 77.5%, while 35% IT professionals felt stressful symptoms in.[12] Forty seven percent of data operators reported at least one visual strain symptoms (tired eyes, head aches, impaired visual performance, red or sore eyes) in the last year; 9% reported all four symptoms. Fourty six percent of data operators believed their symptoms were work- related. Looking at the computer for a long time (26%), poor screen quality (14%) and poor environmental conditions (11%) were reported as possible causes.[8] About 30-40% of the employees working in the call center has complaints of eye problems, soreness, dryness, blurred vision, light sensitivity, head ache and all these put together is labeled as the computer vision syndrome.[9] Pyschosocial and organizational factors were related to the experiences of psychological stress, musculoskeletal disorders and problems with vision among computer users.[38],[39] One study found that a high incidence of neck, wrist and back complaints, headaches and eyestrain stemmed from exceptionally long periods of sitting with neck flexed and looking at the computer screen in a finance auditing job.[40] The report of symptoms of pain in neck, shoulder and hand wrist were reported in call center workers of Brazil.[41] The earlier study[42] raises issues about the importance of psychosocial and organizational factors and employee welfare in the call center-working environment. Conclusions Musculo-skeletal disorders, ocular disorders and psycho-social problems were some of the key health problems observed among IT professionals. There is a need for implementation of the programs that include the concepts of ergonomics, health education, training of personnel to prevent and overcome the morbidity, as well as psycho-social problems among workers in ITES.References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06044t1.jpg] |
| |||||||||

{kind=link}