 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 60, No. 8, August, 2006, pp. 311-317 ORIGINAL CONTRIBUTIONS COMPARISON OF PERINATAL OUTCOME OF GROWTH-RESTRICTED FETUSES WITH NORMAL AND ABNORMAL UMBILICAL ARTERY DOPPLER WAVEFORMS Malhotra Neena, Chanana Charu, Kumar Sunesh, Roy Kallol, Sharma JB Departments of Gynecology and Obstetrics, All India Institute of Medical Sciences, New Delhi Code Number: ms06045 Abstract AIMS : To evaluate the role of umbilical artery Doppler in growth- restricted fetuses.MATERIALS AND METHODS: In a prospective observational study, 70 pregnant women with growth-restricted fetuses confirmed by ultrasound, were followed up with Doppler studies of the umbilical artery. The study group consisted of 35 women, where the Doppler waveform in the umbilical artery was compromised (either absent end diastolic flow [AEDF] or reversed end diastolic flow [REDF]). These were compared with an equal number of controls, where growth- restricted fetuses had normal doppler waveforms. Outcome measures were evaluated in both groups and analyzed. RESULTS: The periods of gestation at delivery were 27.2 ± 3.5 weeks in group 1 and 37 ± 3.3 weeks in-group II, respectively. Perinatal morbidity and mortality was significantly increased in the group with compromised umbilical artery blood group. Birth weight in group I was 742 ± 126 grams and in group II was 1680 ± 259 grams. This difference was statistically significant (P=0.0001). In comparison to AEDF, REDF fetuses had more morbidities. Perinatal mortality was also significantly increased in this group (P=0.001). CONCLUSION: Umbilical artery Doppler should be used in the management of growth-restricted fetuses. In those fetuses in normal Doppler, pregnancy can be prolonged. REDF is an indication for termination of pregnancy. Keywords: Pregnancy outcome, ultrasonography, prenatal, blood flow velocity, fetal growth retardation Intrauterine growth restriction (IUGR) is a syndrome, characterized by failure of the fetus to attain its normal growth potential; fetuses with IUGR, therefore represent a subset of fetuses designated small for gestational age (SGA). IUGR is associated with significant morbidity in the form of meconium aspiration syndrome (MAS), hypoglycemia, hyaline membrane disease (HMD), early onset sepsis (EOS), intrapartum asphyxia, delayed milestones and stillbirths in extreme cases. The use of Doppler ultrasound has helped in better management of these patients. In the most extreme waveform abnormality, there is reversed (REDF) or absent end diastolic flow (AEDF), which is considered a very ominous sign of placental compromise and is associated with high perinatal mortality rates.[1],[2],[3] There are still several clinical problems subsequent to the detection of these severe hemodynamic pathologies. These include the consideration of etiological factors, prognostic evaluation of the fetus and the timing of the delivery. These problems are of special importance in cases where doppler flow abnormalities are detected in the late- second or early-third trimesters.[4] The aim of this prospective study was to compare perinatal outcome in forms of diagnosis-delivery interval gestational age, at delivery birth weight, neonatal intensive care admissions, respiratory distress syndrome and other morbidities and mortalities in patients with a normal umbilical artery flow, as compared to those with absent/reversed diastolic flow in the umbilical artery. We also tried to determine the time interval for which the pregnancy could be prolonged after AEDF set, in extreme premature fetuses without an increase in the perinatal mortality. MATERIALS AND METHODS The study population consisted of 70 women who had singleton pregnancies with small for- gestational-age fetuses. These women either attended the Antenatal clinics with us or were referred in view of IUGR over a period of 5 years (from 2001-2005). The pregnancies were dated by a combination of last menstrual period and first-trimester-dating scan.The diagnosis of severe intrauterine growth-restriction was made clinically and confirmed subsequently on ultrasound, when the fetal abdominal circumference was below the third centile. A detailed anomaly scan was performed on all fetuses and dysmorphic fetuses were excluded from the study. Karyotypically abnormal fetuses were also excluded from the study, besides patients with a positive TORCH test on screening. Mothers with chronic hypertension and preeclampsia were excluded from the study group. In other words, patients with idiopathic intrauterine growth retardation were included in the study. All women included in the study, were subjected to umbilical artery doppler measurements in addition to growth parameters, liquor and placental grading. The women were divided into two groups depending on their doppler findings. Group I (n=35) comprised of women with intrauterine growth restriction, with absent or reversed diastolic flow in the umbilical artery. The other group II (n=35) included women with small-for-date fetuses, with normal umbilical artery doppler flow. Each woman was given a course of steroids (intramuscular betamethasone 12 mg, 2 doses and 24 hours apart). Clinical anthropometry was done every week on the mothers. Fetal biometry to evaluate growth was done fortnightly. Uterine artery doppler was performed at the baseline and fetuses were evaluated weekly/biweekly with the same, to decide management. Intensive fetal monitoring was performed with non stress test (NST), liquor estimation on ultrasound and biophysical profile (BPP). The frequency of these tests varied on the intensity of growth restriction, as judged in biometry and umbilical artery doppler. With worsening, Doppler remote from term fetuses were monitored with NST and BPP every day. Decision to deliver was taken in situations as:
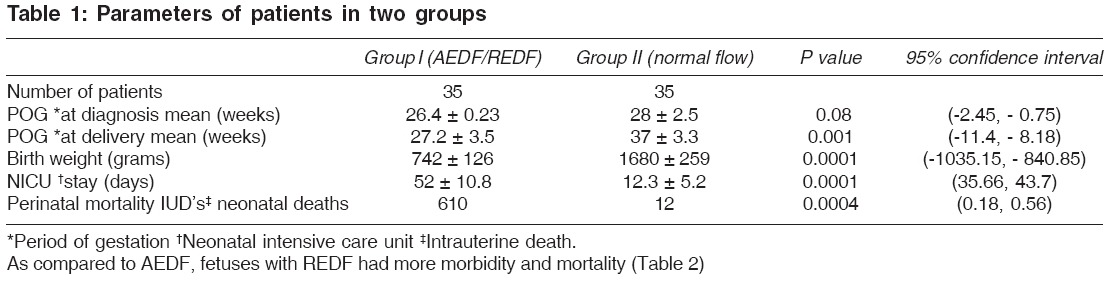
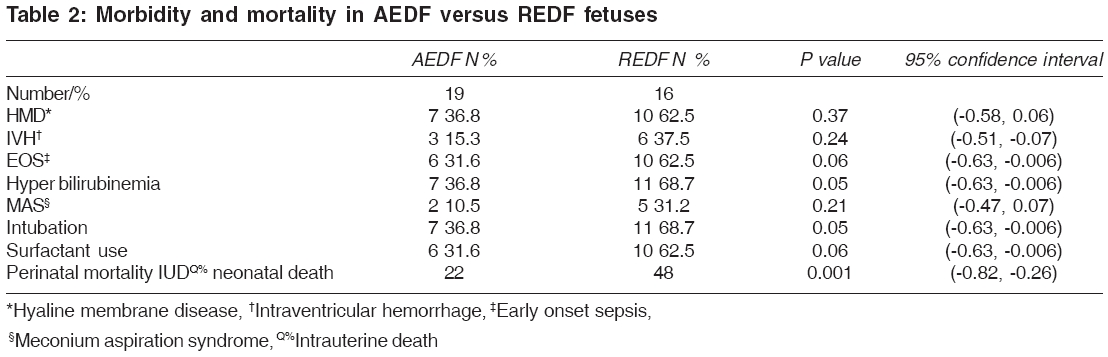
Outcome data were collected. They included diagnosis to delivery interval, gestational age at birth, admission to neonatal intensive care unit (NICU), duration of NICU stay, duration of hospital stay and morbidity and mortality if any. The results were analyzed. Statistical methods The data was examined on the univariate basis to determine crude odds ratio for each variable of interest. Statistical significance was established by means of chi-squared test, Yale′s correlation or Fischer′s exact test for small expected frequencies. The confidence limits of the odds ratio were calculated by means of the method of Cornfield. RESULTS The mean age of patients in group I ranged from 26 ± 3.2 years and that of patients in Group II ranged from 28 ± 2.7 years, which was comparable. Ten women in each of the groups were pregnant for the first time. Seven patients in group I had intrauterine deaths in the previous pregnancies. Various parameters of group I and II are shown in [Table - 1]. Absent end diastolic flow (AEDF)/reversed end diastolic flow (REDF) was diagnosed at a gestational age of 27.4 ± 0.23 weeks in group 1. In patients with REDF, delivery were conducted within a few hours (7.5 ± 2.8). However, in patients with AEDF, pregnancy could be prolonged for a few days (10.8 ± 3.7 days) with intensive fetal monitoring. This was helpful in women, where time was needed to administer betamethasone or in those women who were remote from the threshold of maturity, that is around 26 weeks gestation until 30 weeks. Women with IUGR, with a normal flow were delivered at a gestation of 35 ± 2.8 weeks. Difference in birth weight of babies in the two groups was statistically significant ( P =0.0001), as was the neonatal intensive care unit stay (0.0001). Morbidity, namely HMD, intraventricular hemorrhage (IVH), MAS, EOS and hyperbilirubinemia were more in group I. The perinatal mortality in group I was 45.7%, as opposed to 8.5% in group II. This difference was statistically significant ( P =0.0004). As compared to AEDF, fetuses with REDF had more morbidity and mortality [Table - 2] DISCUSSION Doppler usage has guided obstetric decision- making, particularly in growth-restricted fetuses. Controversy continues as to which is the best fetal vessel for deciding pregnancy continuation, vis-à-vis termination. Evidence from authorities[5] recommend umbilical artery Doppler to be good, but supplementation of other vessels such as middle cerebral artery (MCA) or ductus venosus, may add value to decision-making. Ductus venosus waveforms are time- consuming and may not be possible for all sonographers. Ductus venosus and all venous assessment should be performed by skilled ultrasonographers. It provides the preload situation of the fetal cardiac system. Moreover, changes in MCA territory may reflect advanced stages of fetal hypoxia, where many fetuses may not be salvageable. For all these reasons, umbilical artery doppler is preferred in clinical settings. The pregnancies most likely to benefit from the use of umbilical artery velocimetry, are those with a presumption diagnosis of IUGR, whether as an idiopathic process or in the presence of placental insufficiency. Several studies have been carried out to prove the role of umbilical artery doppler in high-risk pregnancy. It is thought that in conditions like pre-eclampsia, narrowing of small uteroplacental vessels causes an increased vascular resistance, which in turn reflects as abnormally high index valves or even AEDF/REDF.[6],[7] Many authors have found a correlation between acidosis and hypoxia in the blood obtained from pregnancies with AEDF/REDF. Moreover, in fetuses with a compromised umbilical artery diastolic flow, an extremely low cerebral artery vascular resistance exists and sudden cerebral hyperperfusion may occasionally occur, leading to cerebral hemorrhage.[8] Permanent damage to the central nervous system due to increased placental impedance, may account for neurodevelopemental deficits seen in growth- restricted fetuses from pregnancies with utero-placental insufficiency. Various studies have confirmed the clinical benefits of umbilical artery doppler velocimetry in high risk pregnancies, where this method has been compared with conventional NST, BPP and ultrasound fetometry. Doppler studies also allow more precise targeted prenatal monitoring and obstetric interventions, as pathological Doppler findings may be detected several hours to days before any abnormality, in cartiotocographic tracings.[9],[10] The problems in clinical practice do not end with detection of an abnormal doppler pathology. The time between the detection of AEDF flow in the umbilical artery and occurrence of abnormal fetal heart rate patterns varies greatly, causing ambiguity in the subsequent decision-making. The magnitude of the problem considerably increases in cases where extreme prematurity and imminent fetal asphyxia are coexistant. The result of the present study clearly demonstrated the efficacy of doppler in predicting fetal outcome. The perinatal mortality in women with AEDF/REDF was 40%, in contrast to 10% in women with normal doppler findings. Morbidity of fetuses, namely MAS, HMD, IVH, prematurity, oligohydramnios, SGA and EOS hyperbilirubinemia, were all higher in fetuses with AEDF/REDF. Our results are comparable to various previous studies.[11],[12],[13],[14],[15],[16] In a large study on 145 growth restricted fetuses from Italy, Cosmi and co-workers[17] reported that neonatal death was increased in fetuses with umbilical artery reversed flow ( P < .05). They also concluded that fetuses with idiopathic growth restriction, low birth weight, umbilical artery reversed flow and ductus venosus absent or reversed flow, had an increased perinatal morbidity and mortality. Schwarze et al ,[18] after analyzing 74 growth-restricted fetuses between 24 to 34 weeks of gestation, concluded that abnormal venous Doppler waveforms in preterm IUGR fetuses with ARED flow, are strongly related to adverse fetal and perinatal outcomes before 32 weeks of gestation. Gerber et al . studied[19] the short-and long-term morbidity and mortality among children associated with abnormal umbilical artery Doppler and concluded that IUGR associated with umbilical Doppler AEDF/REDF does not show any benefit from an expectant management in terms of long-term morbidity, in addition to being associated with an increased perinatal loss. The decision to continue or deliver fetuses in the presence of AEDF is perplexing for the treating obstetrician. However, we noticed that the pregnancy could be continued even in the presence of AEDF for appoximately 10 days, with intensive fetal surveillance. This may provide time for administration of steroids to enhance fetal lung maturity and also the extra 10 days may add to the fetal weight. This time also enables for shifting of the patient to a tertiary centre where proper neonatal care can be provided. To conclude, the present study recommends the use of doppler in all patients of IUGR. If end diastolic flow is normal, we can wait and repeat Doppler regularly along with other methods of fetal surveillance like NST and BPP, as the women with normal doppler findings had very low perinatal morbidity and mortality. But in women with AEDF/REDF, if the baby is salvageable and nursery facilities are available, it is safer to deliver the baby for a better perinatal outcome, as the number of perinatal deaths were very high in this group. Delivery can be delayed by 1-2 weeks if desired, with very intensive fetal surveillance in cases of AEDF, but immediate delivery is advocated when REDF sets in. REDF is a terminal event associated with an extremely high perinatal mortality. We are of the opinion that doppler studies should be done for all patients with IUGR, but larger follow-up studies are required to confirm the same and also to follow the long term consequences on the fetus. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06045t2.jpg] [ms06045t1.jpg] |
| |||||||||

{kind=link}
{kind=link}