 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
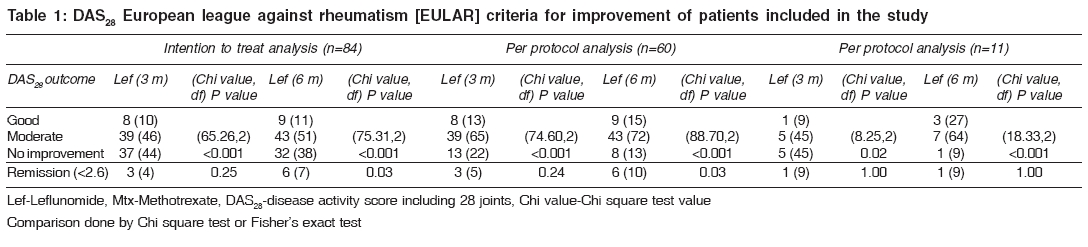
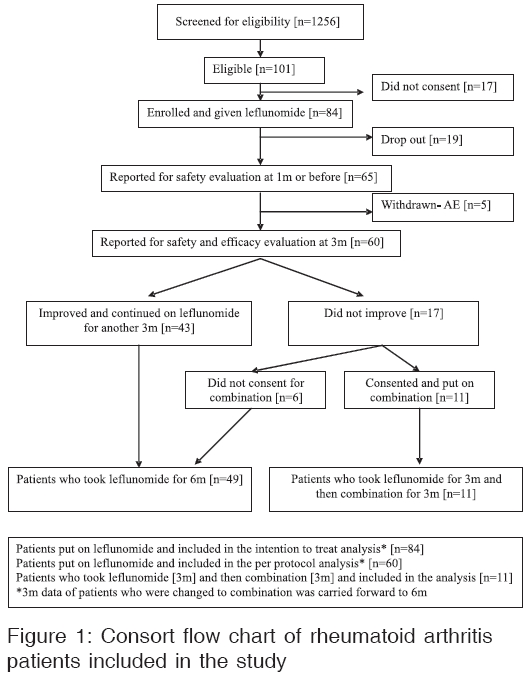
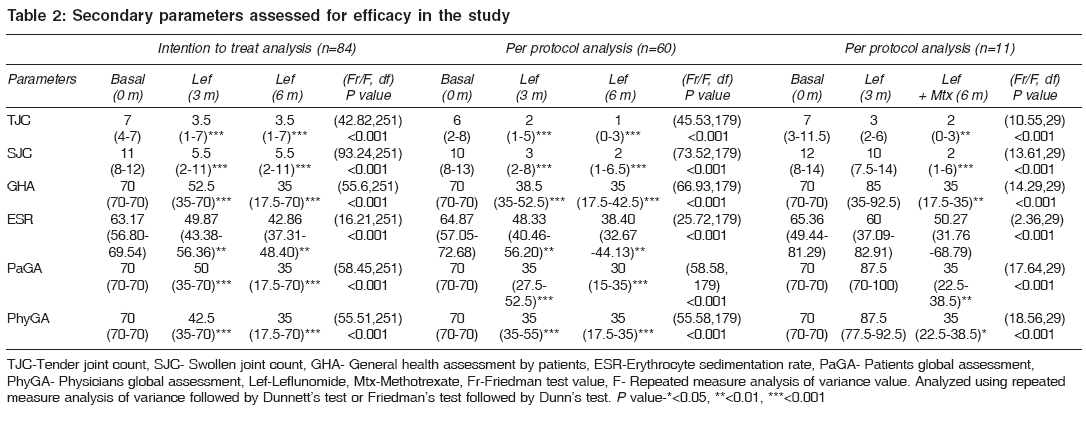
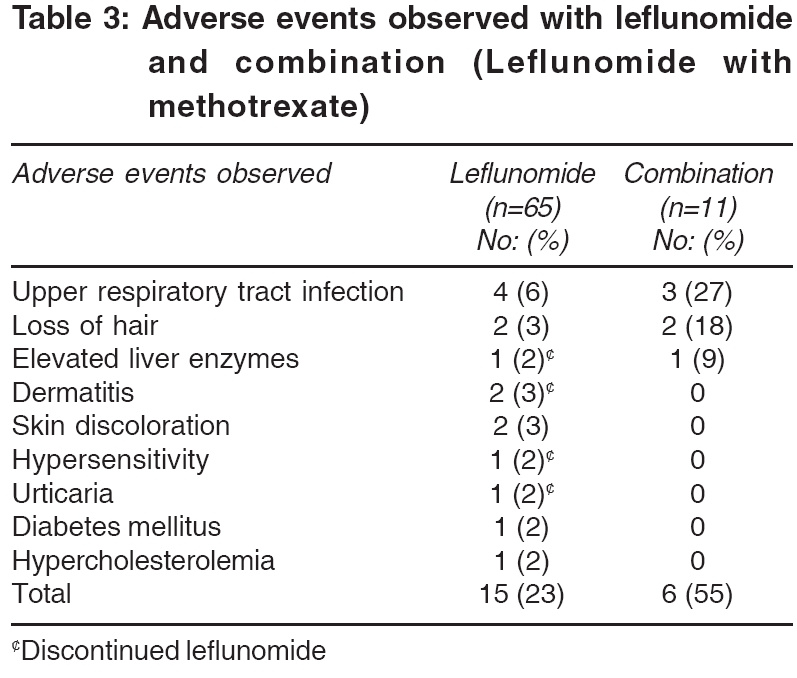
Indian Journal of Medical Sciences, Vol. 60, No. 8, August, 2006, pp. 318-326 ORIGINAL CONTRIBUTIONS EFFICACY AND SAFETY OF LEFLUNOMIDE ALONE AND IN COMBINATION WITH METHOTREXATE IN THE TREATMENT OF REFRACTORY RHEUMATOID ARTHRITIS T. ANTONY, V. M. JOSE, B. J. PAUL*, T. THOMAS Department of Pharmacology and *Rheumatology Division of Medicine Department, Government Medical College, Calicut, Kerala, India Code Number: ms06046 Abstract BACKGROUND: Rheumatoid arthritis patients who develop refractoriness are left with no alternatives other than leflunomide and costly biological response modifiers. Leflunomide, though effective, was associated with adverse events and has not been extensively studied in the Indian population.AIMS: Determination of safety and efficacy of leflunomide alone and if not useful, in combination with methotrexate in patients refractory to conventional disease-modifying agents. SETTING AND DESIGN: Open labeled clinical trial with leflunomide [100 mg, OD x 3 days followed by 20 mg, OD x 6 months], if no improvement at three months, combined with methotrexate [5-7.5 mg, OD x 3 months] at a tertiary care hospital. MATERIALS AND METHODS: The primary endpoint in the improvement in EULAR criteria and secondary endpoints were patient and physician global evaluation, incidence of remission and biochemical and clinical adverse events. STATISTICAL ANALYSIS: Chi square test or Fisher's exact test and parametric and non-parametric repeat measure ANOVA were used for analysis. RESULTS: Among 84 patients who were included in the study, leflunomide showed improvement and remission in 52 [62%] and 6 [7%] in six months, by intention to treat analysis. Adverse events were observed in 15, discontinuation in 5 and 24 dropped out. With combination in 11 patients, there was improvement and remission in nine [91%] and one [9%] after three months. Adverse events were observed in six and one discontinued. CONCLUSIONS: If regular monitoring of hepatic function and hematological parameters are performed, leflunomide is an effective and safe drug in the Indian population in resistant rheumatoid arthritis patients, especially if used alone. Keywords: DAS28, EULAR, humans, leflunomide, methotrexate, refractory, rheumatoid arthritis, drug therapy Rheumatoid arthritis (RA) if left untreated, ultimately causes functional impairment.[1] Non-steroidal anti-inflammatory drugs (NSAIDs) help only in symptomatic relief, corticosteroids have problems with chronic use and disease-modifying anti-rheumatic drug (DMARD) use leads to refractiveness and toxicity.[2],[3],[4],[5] Leflunomide has shown good promise, but adverse events have been a limiting feature, especially in combination with methotrexate.[6],[7] No other affordable drugs are available for refractory patients in the Indian scenario.[3] The present study was aimed at determining the efficacy and safety of leflunomide in patients refractory to conventional DMARD and if there is unsatisfactory response after three months, then in combination with methotrexate for another three months. MATERIALS AND METHODS RA patients of all American College of Rheumatology (ACR) classes of either sex between 18 and 65 years, refractory to conventional treatment as per our hospital protocol, were included in the study.[1],[8] The refractory RA patients were those who could not be controlled satisfactorily by chloroquine (150 mg base / day daily) or hydroxychloroquine (200-400 mg/day once or twice daily), depending on affordability and sulphasalazine (1.5-3 gm/day twice or thrice daily) and methotrexate (7.5-25 mg/week) after three to six months use of each, due to lack of efficacy or adverse drug reaction. Patients with uncontrolled hypertension, hepatic, renal, pulmonary and hematological disorders, overlap syndrome, pregnant, lactating and patients of the reproductive age group who were not ready to practice contraception, were not included in the study. This was an open labeled clinical trial conducted from February 2002 to August 2003, at the Rheumatology Clinic of a tertiary care center in accordance with the Declaration of Helsinki, following approval by the institutional ethical committee. The first author gave the drugs, while evaluation was performed by the third author (rheumatologist). Patients were given a wash out period of two weeks, during which NSAIDs and proton pump inhibitors were allowed. Patients on prednisolone were tapered to a maximum of 10 mg or less per day. No increase in prednisolone, initiation of NSAID or increase of NSAID dose, was allowed during the study. Patients were given leflunomide-100 mg for the first three days, followed by 20 mg daily for the next three months. Those who worsened on the patient′s or physician′s general health assessment, were given the option for adding weekly methotrexate (5-7.5 mg) for three months. Compliance was assessed by pill counting. Tablet leflunomide 20, 100 mg (Cipla Pharmaceuticals Limited) and tablet methotrexate 2.5 mg (Cipla Pharmaceuticals Limited) were used for the study. The European league against rheumatism (EULAR) criteria of improvement according to DAS 28 , was considered as the primary efficacy variable.[9],[10] [Table - 1] The physician′s and patient′s global assessment, incidence of remission and biochemical and clinical adverse events were the secondary parameters. Patients with DAS 28 score < 3.2, 3.2-5.1 and> 5.1 were considered to have mild, moderate and high severity disease. We considered even minimal worsening of the patient or physician assessment as an indication for combination therapy, since we felt that personal satisfaction was more important than the DAS 28 score. Safety parameters assessed included blood pressure, body weight, hemoglobin, packed cell volume, red, white and platelet cell counts, creatinine, aspartate aminotransferases (AST), alanine aminotransferases (ALT), alkaline phosphatase, protein and albumin at the baseline, first, third and sixth months. Any clinical events which affect the patient adversely, were recorded as adverse events. To determine the efficacy of leflunomide with 95% precision and 10% variability, considering efficacy to be 76%, the sample size required is 70 patients. Intention to treat analysis (ITT) and per protocol analysis (PP) were performed. Eleven patients put on combination were analyzed separately, as well as they were part of the ITT and PP analysis with their three month data forwarded to the sixth month. In case of missing values, the last value was carried forward. The data was analyzed using Chi square test or Fischer′s exact test; Friedman′s test followed by Dunn′s test; or repeated measure analysis of variance followed by Dunnett′s test. Values were expressed as numbers, percentages and mean with 95% confidence interval or median with inter quartile range, whichever was appropriate. RESULTS Of 1256 patients screened, 101 were eligible for the study [Figure - 1]. ITT included 84 patients of which 66 (79%) were females who had a mean age of 48.92 (46.49-51.35) years, mean arthritis duration of 90.32 (74.09-106.56) months, with 8 (10%), 43 (51%) and 33 (39%) patients having ACR class I, II and III disease. PP analysis included 60 patients of which 52 (87%) were females who had a mean age of 48.67 (46.15-51.19) years, mean arthritis duration of 97.45 (76.46-118.44) months, with 4 (7%), 34 (57%) and 22 (37%) patients having ACR class I, II and III disease. The combination group included 11 patients of which 10 (91%) were females who had mean age of 45.36 (39.32-51.41) years, with mean arthritis duration of 99.27 (64.49-134.06) months having 0, 8 (73%) and 3 (27%) patients with ACR class I, II and III disease. Twenty four patients on leflunomide and four patients on combination were on prednisolone and all 84 patients on leflunomide were taking NSAIDs. EULAR criteria showed improvement in a significant number of patients put on leflunomide [Table - 2]. Zero, 7 (8%), 77 (92%) and 0,6 (10%), 54 (90%) patients with mild, moderate and high disease severity respectively, were included in the ITT and PP analysis. Twenty (24%), 45 (54%), 51 (61%) and 12 (20%), 37 (62%), 38 (63%) patients at baseline, 3 and 6 months showed rheumatoid factor negativity by ITT analysis (Chi value=25.91, df=2, P < 0.001) and PP analysis (Chi value=28.97, df=2, P < 0.001), respectively. Secondary efficacy parameters also improved from three months [Table - 3]. Fifteen adverse events were noted in 65 different compliant patients. Lab parameters showed no significant difference. AST and ALT were raised and was 1.2 to ≤ 2 times the Upper Limit of Normal (ULN) in 27 (42%) and 22 (34%), 2 to ≤ 3 ULN in 2 (3%) and 5 (8%) and to> 3 ULN in 1 (2%) and 3 (5%), respectively. A significant number of patients improved as per the EULAR criteria [Table - 2], after three months of combination use. Zero, 1 (9%) and 10 (91%) patients at the baseline, had disease of mild, moderate and high severity. Zero, 5 (45%) and 6 (55%) patients were rheumatoid factor negative at the baseline, 3 and 6 months (Chi value=8.46, df=2, P =0.01), respectively. Most secondary efficacy parameters improved with three month combination use [Table - 2]. Six adverse events were noted in 11 different patients put on combination therapy [Table - 3]. Lab parameters showed no significant difference. AST and ALT were raised 1.2 to ≤2 times ULN in 1 (9%) and 4 (36%) patients and> 3 times ULN in 1 (9%) and 1(9%) patients, respectively. EULAR non-responders with leflunomide when compared with responders, showed no significant difference of age, duration of arthritis, duration of morning stiffness, body weight, female gender, ACR class or basal rheumatoid factor negativity. DISCUSSION EULAR criteria showed improvement with leflunomide in 47 (56%) and 52 (62%) patients, while remission was seen in 3 (4%) and 6 (7%) patients at three and six months respectively, as per ITT analysis. PP analysis showed improvement in 47 (78%) and 52 (87%) patients, while remission was seen in 3 (5%) and 6 (10%) patients at three and six months, respectively. A significant number of patients derived benefit from the three month treatment. Efficacy ranging from 50 to 87% with monotherapy using various assessment criteria, have been observed in studies in different situations to date, irrespective of the absence of the loading dose.[5],[6],[7],[11],[12],[13],[14],[15],[16],[17] Hematological and biochemical parameters showed no significant change. Few patients had liver enzyme elevation, though it did not reach significance and only one had to discontinue. Earlier studies have shown liver enzyme elevation, which subsequently normalized.[6],[7],[15],[16],[17] Twenty four (29%) patients dropped out of the study and an adverse event was observed in 15 patients, of which five withdrew. Skin reactions observed were more of type B adverse event, which were unpredictable.[18] Adverse events could have been due to worsening of RA and unrelated events also, as was seen in an earlier study.[17] Leflunomide has shown adverse events in up to 79%, withdrawal due to adverse events in up to 22%, hepatic enzyme elevation in up to 11%, withdrawal due to elevated hepatic enzyme in up to 7.1%, total withdrawal in up to 47% and serious adverse events in up to 5% of patients in various studies.[6],[11],[12],[13],[14],[15],[16],[17] Combination was suggested by worsening physician or patient global assessment, in 17 (20%) patients. The previous bad experience with methotrexate was the reason for non-acceptance of combination by 6 (7%) patients. With leflunomide alone for three months, EULAR criteria showed improvement in 6 (54%) and remission in 1 (9%), respectively. With combination for three months, there was improvement in 9(91%) and remission in 1 (9%), respectively. Efficacy ranging from 46 to 53% with combination therapy using various assessment criteria, has been observed.[5],[6],[7],[11],[12],[13],[14],[15],[16] Hematological and biochemical parameters showed no significant difference with combination use. At one month, there was a decrease in red, white and platelet cell counts, probably due to marrow toxicity. However, it soon reverted and was not clinically significant at any stage. Adverse events were observed in 6 of 11 patients and one had to discontinue, due to elevated hepatic enzymes. Leflunomide in combination with methotrexate has shown adverse events in 89% and 155 adverse events in 29 patients in two studies, withdrawal due to adverse events in up to 12.3%, hepatic enzyme increase in up to 63%, withdrawal due to increase in hepatic enzymes in up to 10% and total withdrawal in up to 23%.[7],[15],[16],[19] There was 32 and 63% patients showing more than 1.2 times the basal hepatic enzyme increase.[7],[15],[16] We had only 11 patients to compare with these studies for combination therapy and found that the combination was a reasonably safe and effective option. Leflunomide alone has shown efficacy in 2 and 5 year clinical trials and was not associated with loss of efficacy with continuous use.[20],[21],[22] Quality of life studies, X-ray evaluation and maximal signal intensity enhancement by dynamic gadolinium- enhanced magnetic resonance imaging, have supported its efficacy.[23],[24],[25],[26] It was shown to be effective and safe in general practice.[27] Weekly use and even omitting the loading dose, has shown comparable efficacy to daily use, with fewer adverse events.[17],[28],[29] It was effective in combination with methotrexate, though incidence of adverse events, especially hepatotoxicity, was high.[7],[15],[17],[19] Post-marketing surveillance has shown leflunomide to be a safe drug.[30] It was also shown to be not more associated with hepatotoxicity, compared to other DMARD′s.[7],[15],[19],[31] This was an open label study. However, the evaluation was done by the rheumatologist along with the chief investigator, which should have decreased the bias. No prognostic factors which predict response to leflunomide, could be identified from the study.[32] Including only refractory patients would have underestimated the efficacy, however, considering the novel mechanism of action of leflunomide, this can be expected to be minimum. Further, including refractory patients alone will give the efficacy in pragmatic situations, which is the more likely situation it is expected to be used in practice. There is definitely need of a larger study with combination to confirm the efficacy and safety. We observed a high incidence of drop outs, adverse events-some leading to withdrawal, elevation of hepatic enzymes and satisfactory efficacy with leflunomide. Considering the refractory nature of the patients included and lack of an alternative treatment and financial constraints, leflunomide can be considered an effective and safe option in the Indian population in resistant RA, provided regular monitoring of liver function and hematological parameters are performed. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06046f1.jpg] [ms06046t1.jpg] [ms06046t2.jpg] [ms06046t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}