 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
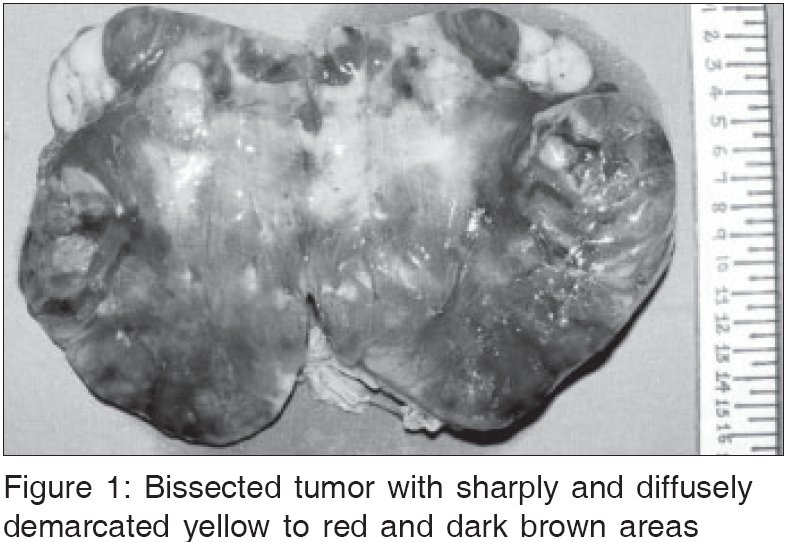
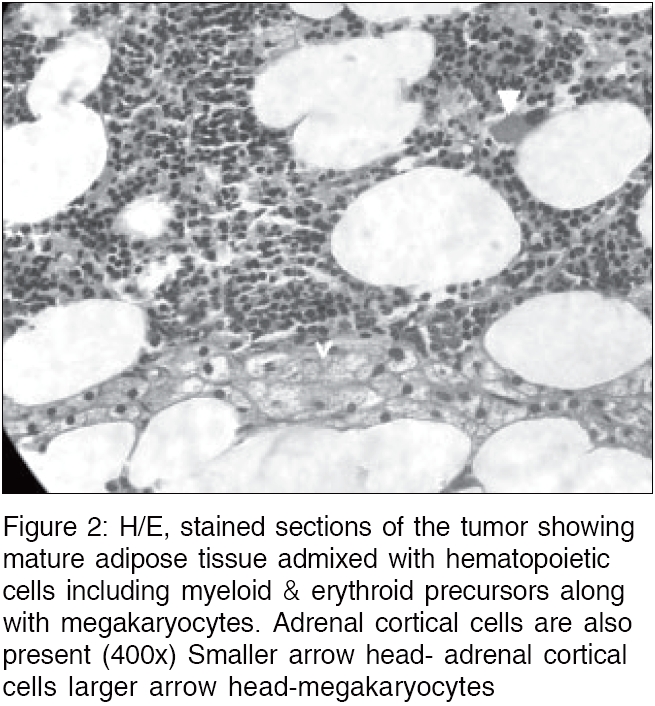
Indian Journal of Medical Sciences, Vol. 60, No. 8, August, 2006, pp. 331-333 Letter To Editor CATECHOLAMINE SECRETING ADRENAL MYELOLIPOMA Hema Tamidari, Anand Kumar Mishra*, Sushil Gupta**, Amit Agarwal*** Department of Surgery, KEM Hospital, Mumbai, *Department of Endocrine and Breast Surgery, Departments of **Endocrinology, ***Endocrine and Breast Surgery, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raibareli Road, Lucknow - 226 014, India Code Number: ms06049 Sir, We report a patient with biochemically proven pheochromocytoma, whose histology of a resected adrenal mass revealed adrenal myelolipoma, raising queries about this association. A 48 year female presented with right upper quadrant abdominal discomfort, regurgitation and occasional anxiety attacks associated with sweating and diabetes mellitus, for 45 days. She was known to be hypertensive for 12 years, controlled on beta-blockers. Her BP was 140/80 mm of Hg, with no postural drop. Abdominal examination revealed a vague, ill-defined, retroperitoneal lump in the right hypochondrium. CT abdomen revealed a 11 x 10.5 x 7 cm, well- encapsulated, non-homogenous, low density (-100 to -200 HF units), right adrenal mass with normal left adrenal gland. Serum potassium (4.2 meq/l), basal cortisol and low dose and high dose dexamethasone suppression tests were normal (22.5, 0.5 and 0.5 micro gm/dl, respectively). The 24 hour urinary metanephrine was 2.86 mg/day (normal-less than 0.8). DHEAS and testosterone estimation was not done, as there was no suspicion of malignancy. Thus, a diagnosis of pheochromocytoma was made and the patient was prepared with an alpha blocker (Prazosin 10 mg/day for 13 days). A beta blocker (Propanolol 80 mg/day) was added on the 10th day. She was explored via the anterior transperitoneal subcostal approach. A 13 x 11.7 cm well- encapsulated right adrenal tumor (weight: 575 gm) was excised. Hemodynamically, the patient was stable intra-operatively. The cut surface showed fatty content which was bright yellow in colour [Figure - 1]. Histopathology [Figure - 2] revealed myelolipoma with no evidence of pheochromocytoma or medullary hyperplasia. Our pathologist looked for medullary hyperplasia with specific immunohistochemical staining by chromogranin A, but there was no evidence of it. The patient became normotensive immediately following surgery and the 24- hour urinary metanephrine collected on the 10th post-operative day was 0.63 mg/day (normal). In the follow-up of 14 months, the patient was normotensive and her blood sugar was normal. Myelolipoma is an uncommon benign tumor of the adrenals, occurring in 0.08 to 0.2% of autopsy series.[1] Adrenocortical dysfunction occurs in 10% and may present as Addison′s disease, Cushing′s disease, hermaphroditism, virilism, extreme obesity or multiple endocrinopathy. Associated hypertension is either incidental or due to mechanical compression on the renal vessels by the tumor. Rocher et al have reported pheochromocytoma with a myelolipoma on the contra-lateral side,[2] while Ukimura et al[3] reported a case with co-existence of the two lesions as histologically separate areas within same gland. Ishay et al have reported combined adrenal myelolipoma and medullary hyperplasia.[4] In our patient, we suspected myelolipoma on the established CT criteria of a well-circumscribed, non-homogenous mass containing fat localized to the adrenal gland with low attenuation values (-100 to -200) and pheochromocytoma on biochemical evidence, but no evidence on histopathology, has no explaination. The cure of hypertension and diabetes in follow-up are the only clinical parameters which suggest that the mass was functioning. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06049f1.jpg] [ms06049f2.jpg] |
| |||||||||

{kind=link}
{kind=link}