 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 60, No. 8, August, 2006, pp. 334-344 Practitioners section PREGNANCY AND RHEUMATOID ARTHRITIS VISHAL R.TANDON, SUDHAA SHARMA*, ANNIL MAHAJAN**,VIJAY KHAJURIA, AJAY KUMAR Post Graduate Departments of Pharmacology and Therapeutics, *Obstetrics and Gynecology, **General Medicine, Govt Medical College, Jammu, India Code Number: ms06050 Abstract Pregnancy in most cases, is associated with remission of rheumatoid arthritis (RA), but a quarter of patients continue to have active disease or even worsening of the disease and most patients who improve, relapse in the postpartum period. The pathophysiology of this improvement in disease activity during pregnancy remains unknown, but hormonal, cell-mediated immunological and humoral immunological changes during pregnancy, have been proposed responsible for this. Most of the pregnant women with RA have an uneventful course, with no significant complications. In general, no significant increase in maternal or fetal morbidity seems to be attributable to RA. Patients with RA do not have decreased fertility. A majority of patients with RA may go in remission and anti-rheumatic treatment may not be required as soon as women become pregnant. But other patients who continue with the disease activity require treatment. The preferred disease-modifying agents during pregnancy are sulfasalazine and hydroxychloroquine. Azathioprine and cyclosporine can be used if the benefits outweigh the risks. Paracetamol and low dose prednisone are preferred and considered safe, both for mother and fetus. Methotrexate and lefunomide are contraindicated and must be prophylactically withdrawn before a planned pregnancy. Biologics generally should be stopped when pregnancy is discovered. An overall rational approach is highly warranted to treat RA during pregnancy.Keywords: humans, pregnancy, rheumatoid arthritis, (physiopathology or physiology) Pregnancy has an important impact on rheumatoid arthritis (RA) and on many other rheumatic diseases like systemic lupus erythematous, Sjogren′s syndrome, juvenile idiopathic arthritis, Reiter′s syndrome, scleroderma, dermatomyositis / polymyositis and psoriatic arthritis.[1],[2],[3] It is well known that females suffer more of musculo-skeletal and rheumatic complaints, including RA.[4] RA is three times more common in females.[5] Because of female predominance of this disease, it is likely that pregnancy will be a question encountered by patients and their practitioners. Hence, it becomes important for practitioners to know the course of RA in pregnancy, effect of RA on outcome of pregnancy for mother and child and fertility and disease management before, during and after the pregnancy. The present review will discuss all these aspects. Pregnancy and rheumatoid arthritis Pregnancy results in an altered immune state which contributes to a change in the course of autoimmune illness, including RA. For decades, the ameliorating effects of pregnancy have been observed on disease activity in women with RA. Dr. Hench[6] in 1931, was the first to make this classical observation. A two to five fold decrease in risk to develop RA during pregnancy in healthy women, has been observed.[1] Retrospective[7] and prospective[8],[9] studies have confirmed improvement in the disease activity of RA. Silman and associates performed a case control study in 1992, with 88 women with RA and reported that pregnancy had a protective effect on disease onset.[10] Pregnancy is often associated with remission of the disease in the last trimester. More than three quarters of pregnant patients with RA, improve in the first or second trimester.[1] The improvement in arthritis during pregnancy tends to be short-lived and most patients who improve, relapse in the postpartum period.[9],[11] Ninety percent of these experience a flare of the disease, with a rise in rheumatoid factor (RF) tire, in the weeks (or 3months) after delivery.[1] Risk of RA onset during postpartum, usually persists for the subsequent 9 months.[10] It has been reported that rheumatoid arthritis is 5 times more likely to develop after delivery, than at any other time.[3] Barrett and co-workers reported in 2000, that a flare is more common if the woman is breast feeding.[12] While most of the patients with RA have some improvement in their symptoms during pregnancy, approximately a quarter of patients continue to have active disease or even worsening of the disease, requiring treatment throughout pregnancy.[13] Pathophysiology: The pathophysiology of improvement in disease activity during pregnancy, remains unknown. Various theories have been proposed. The effect of hormonal changes during pregnancy Serum estradiol, 17-α-hydroxyprogesterone and 11-deoxycortisol increase throughout pregnancy.[14],[15] Corticoids are well known to exert a variety of important anti-inflammatory and immunosuppressant actions, by virtue of which they can cause improvement in the disease activity of RA.[16] Estrogen can decrease the stromal cell production of interleukein-1 (IL-1), IL-6 and TNF-alpha, which are centrally pathognomonic in the pathogenesis of RA.[17] Similarly, progesterone is well known to maintain pregnancy by decreasing T-cell response[18] and exert an anti-abortive effect.[19] This progesterone-mediated immuno-modulatory mechanism may also contribute to amelioration of RA during pregnancy. However, there is no proof that increased levels of steroid hormones improve disease symptoms of RA, since steroid- binding globulins also increase likewise. Similarly, treatments with female sex hormones or oral contraceptives do not improve the course of RA.[13],[20] Thus, the opinion regarding the influence of hormones on symptoms and progression of RA remains controversial and unclear. The effect of pregnancy on cell-mediated immunity (CMI) Pregnancy is characterized by decreased production of T-helper cell (Th1)-associated cytokines like IL-1 and interferon-gamma and increased production of Th2-associated cytokines like IL-4 and IL-10, as well as decreased production of pro-inflammatory cytokines like TNF-alpha and IL-12.[20],[21] This altered cytokine profile may be one of the mechanisms responsible for the ameliorating effects of pregnancy on RA. Two plasma proteins, pregnancy zone protein (PZP) and placental protein-14, also known as glycodelin-A, increase dramatically during pregnancy and are known to act synergistically to selectively modulate T-cell activation.[22] Inhibition of lymphocyte proliferation and activation, a function of the trophoblast to escape the maternal immune response, is also postulated.[23] Recently, one animal study provided direct evidence that pregnancy benefits in experimentally induced arthritis, by attenuating the cellular immune response.[24] The effect of pregnancy on humoral immunity A proportional decrease in immunoglobulin G (IgG) and an elevated serum alpha-2 pregnancy-associated globulin (PAG) level have been postulated.[1],[25] During human pregnancy, an increase has been detected in asymmetrical IgG molecules in serum and those bound to the placenta, which normally releases factors capable of modulating the immune response. Asymmetrical IgG molecules behave as univalent antibodies and therefore act as antigen blockers.[26] Few other mechanisms also have been proposed for the amelioration of RA in pregnancy.[27] Nelson and co workers reported in 1993, that amelioration of disease is associated with a disparity in HLA Class II antigens between mother and fetus. The maternal immune response to paternal HLA antigens may have a role in pregnancy- induced remission of arthritis.[28] Possible causes for flare-up during the postpartum period[11],[1]
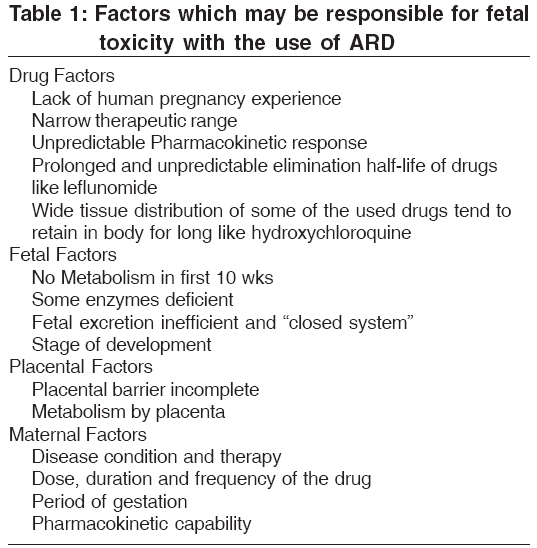
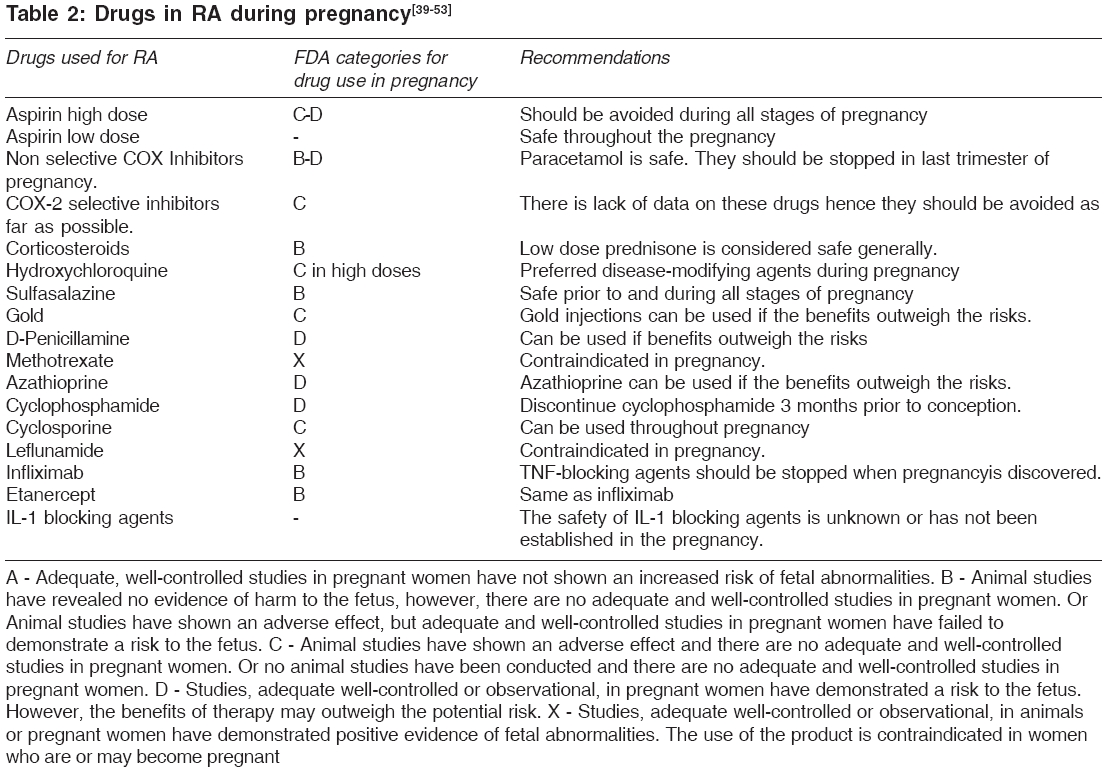
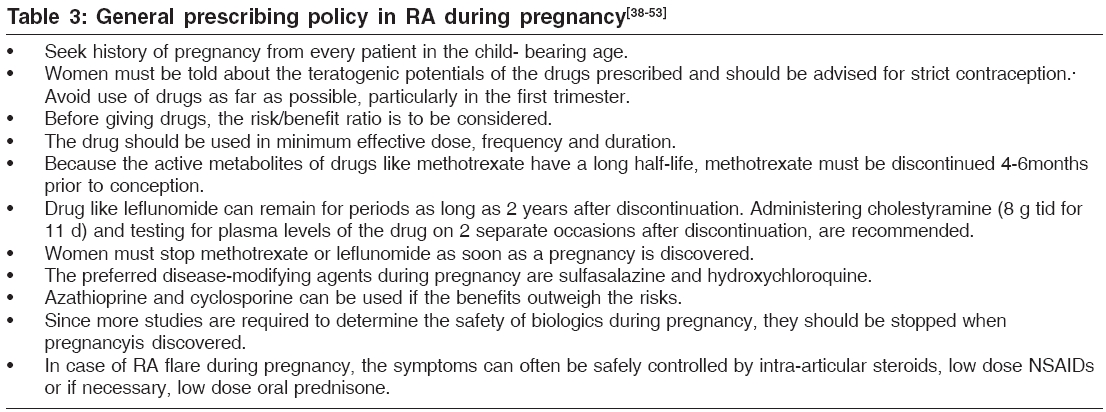
Effect of RA on pregnancy Few studies address the effect of RA on pregnancy. Most women with RA have an uneventful course, with no significant complications. Maternal morbidity during pregnancy and labor in patients with RA is comparable to that of women without RA.[1],[30],[31] However, some contradictory data also exist in the literature with regard to rate of spontaneous abortions and preeclampsia and preterm delivery among pregnant patients with RA.[32] In rare cases, normal vaginal delivery is not possible because of severe hip arthritis. If a caesarean section under general anesthesia is required, special precaution has to be taken about the atlanto-axis subluxation of the spine.[1],[33] Effect of RA on fetal outcome In general, no significant increase in maternal or fetal morbidity seems to be attributable to RA. It does not appear to adversely affect the fetal outcome. Pregnancy loss rate in RA has been recorded (17%), which is similar to a control population of (16%). A case-control study[34] reported premature birth and growth reduction as possible effects of RA, whereas, another study failed to show any adverse fetal outcomes in pregnant patients with RA.[35] Effect of RA on fertility Patients with RA do not have decreased fertility. Most, but not all studies show an increase in nulliparity, whereas parity rates in fertile RA women are unchanged.[36] However, they may require a prolonged time to conceive. Decreased sexual drive, pain, ovulation dysfunction and an impaired hypothalamic-pituitary-adrenal axis may be responsible for these findings.[33] Clinical course[1],[33],[37],[38] Constitutional symptoms of RA may be present. Morning stiffness and fatigue may be diminished and extra-articular manifestations are not increased. Joint pain or stiffness improves in approximately 75% of patients. Decrease in pain as early as in the first trimester, is noticed in most of patients. In some patients, this improvement occurs later, during the second or third trimester. Some patients (16%) achieve complete remission. Nausea, vomiting and morning sickness that occur during the first trimester, may prevent absorption of medications. Pedal edema and back pain that is unrelated to RA, can occur in the later stages of pregnancy. Pallor may be present, as patients with RA can have chronic anemia. Patients on non-steroidal anti-inflammatory drugs (NSAIDs) can develop iron deficiency anemia from gastrointestinal blood loss. Follow up of pregnant rheumatoid arthritis patients Joint examination should be performed to assess inflammatory activity and structural damage. Activity should be assessed by the number of swollen and tender joints. The range of motion of hip and neck joints must be assessed specifically, because patients may need to abduct and externally rotate their hips for vaginal delivery, as well as to identify patients with ligamental instability of the atlantoaxial joint. Assessment should be made for extra-articular symptoms. Examination to assess fetal growth and development as well as maternal health, should be performed according to the obstetrics protocol. Laboratory blood tests are the same as for any pregnancy. The presence of rheumatoid factor does not help predict or correlate with the outcome of arthritis during pregnancy. Erythrocyte sedimentation rate cannot be used to assess RA disease activity during pregnancy, because pregnancy alters the normal values. Closer monitoring of hematocrit values may be required, if patients are on disease-modifying antirheumatic drugs. For sulfasalazine, a complete blood count (CBC), an aspartate aminotransferase assay and alanine aminotransferase assay are required, whereas, for azathioprine, a CBC is required. Radiograph of the cervical spine in patients with persistent neck pain and neurological symptoms is suggested. Ultrasound should be performed to assess fetal well-being according to the obstetrics protocol. A majority of patients with RA may go into remission and anti-rheumatic drugs (ARD) may not be required as soon as the women become pregnant. But other patients who continue with the disease activity require treatment. Many pharmacological principles and factors [Table - 1] must be kept in mind while prescribing antirheumatic treatment, as some drugs carry teratogenic potentials. Drugs used commonly in RA and their status in pregnancy [39],[40],[41],[42],[43],[44],[45],[46],[47],[48],[49],[50],[51],[52],[53] [Table - 2] Aspirin in high dose[39],[41],[42] should be avoided during all stages of pregnancy, particularly in the last trimester, as it can inhibit uterine contractility and prolong labour. It can cause premature closure of ductus arteriosus, kernicterus, hemorrhage and renovascular complications. Aspirin in low dose:[39] ≤80 mg/day appears to be safe throughout the pregnancy without evidence of fetal malformation and clotting problems or premature closure of ductus. On the contrary, it can benefit the patients at risk for pregnancy-induced hypertension and preeclampsia. Non selective COX-Inhibitors:[39],[41],[42] can be used in the first and second trimester of pregnancy if necessary, to control maternal disease. Paracetamol may be considered as a safe analgesic. There is no conclusive report of fetal malformation with the use of NSAIDs. They should be stopped in the last trimester of pregnancy due to associated risks like premature closure of ductus, pulmonary hypertension, impaired renal function and oligohydramnion. COX-2 selective Inhibitors:[39] Theoretically, the effect of COX-2 selective inhibitors on duration of labour and clotting should be less, whereas the effect on fetal vasculature and renal function because of their mechanism, should be equal. However, there is lack of data on these drugs and hence they should be avoided as far as possible. Corticosteroids:[41],[43],[44] are generally considered safe in pregnancy. Low dose prednisone is the preferred drug and is considered safe both for mother and fetus, because placental metabolism by 11-beta hydroxylase limits the exposure of the fetus to the active drug. However, large doses (1-2 mg/kg/day) should be avoided during the first trimester, because of the associated risk of cleft lip and cleft palate.[43] High doses can cause prematurity and intrauterine growth retardation in late pregnancy. In contrast, dexamethasone and betamethasone are fluorinated steroids that are much less metabolized by the placenta. They can have inhibitory effects on physical growth and, long-term alterations in endocrine, immune and neural physiology and should be avoided.[44] Hydroxychloroquine (HCQ):[39],[45] no adverse effects on the child have been found in doses of 200-400 mg/day, commonly used to treat RA. It is thus preferred as the disease-modifying agent during pregnancy, along with sulfasalazine. Because of the long half life and extensive tissue deposition of anti-malarial drugs, discontinuation of therapy at the time of conception or pregnancy does not prevent fetal exposure. Although the trans-placental passage of HCQ has been demonstrated, there is no evidence to support the harm to fetus. In RA patients, the decision to continue or discontinue anti-malarial drugs in pregnancy should be individualized, taking into account the natural remission in pregnancy and exacerbation in postpartum disease. Sulfasalazine:[39],[46] is considered safe in pregnancy, as it does not interfere with conception in women with RA. It can be safely used prior to and during all stages of pregnancy. Gold:[39],[47] In the current prescribing practices, it is prescribed in very few patients. However, injections can be used if the benefits outweigh the risks. D-Penicillamine (DP):[39],[47] should be used if benefits outweigh the risks. If a patient with RA becomes pregnant while receiving DP, the drug should be stopped because of risk of serious congenital deformities, but termination of pregnancy is not indicated. Methotrexate (MTX):[39],[48] is also contraindicated in pregnancy because of its teratogenic effects. Craniofacial defects, anencephaly, hydrocephaly, limb defects and increased rates of abortion have been reported following use of high-dose MTX. The late first trimester appears to be the critical period for these teratogenic effects. Because its active metabolites have a long half-life, MTX must be discontinued 4-6 months prior to conception and treatment with folic acid has to be continued. Strict contraception is needed when the patient is on MTX. Azathioprine:[39] can be used if the benefits outweigh the risks. While fewer women on azathioprine for renal transplant completed their pregnancies, no increase in fetal anomalies has been observed. Women with severe RA that is difficult to control, may use azathioprine during pregnancy. No fetal anomalies are reported with a dose up to 2 mg/kg/day. Cyclophosphamide:[39] Discontinuing cyclophosphamide 3 months prior to conception is recommended. Facial cleft, limb defects and craniofacial dysmorphism has been reported with the use of this drug in the first trimester, whereas, myelotoxicity and growth retardation have been reported in late pregnancy. Cyclosporine:[49] is well studied and can be used throughout pregnancy. Doses of 2-3.5 mg/kg/day, do not increase the risk of pre-maturity or low birth weight. Leflunomide:[39],[48],[50] is a new and effective disease-modifying antirheumatic drug. Animal studies have shown an increased rate of malformations and fetal death in various species, but there is no data on pregnancy outcomes in humans treated with leflunomide. Since the drug has a prolonged and unpredictable elimination half-life, it should be stopped during pregnancy. Because leflunomide can remain for periods as long as 2 years, administering cholestyramine (8 g tid for 11 days) and testing for plasma levels of the drug on 2 separate occasions after discontinuation, are recommended. Without a wash out, the levels of it may stay too high for up to 2 years. Women who wish to conceive have to stop treatment 2 years prior to conception, in case, facilities of drug monitoring or cholestyramine is not available. Otherwise, strict contraception is needed when the patient is on this drug. Infliximab:[51],[52] Pharmacovigilance studies have not shown that the rate of normal live births, miscarriages and therapeutic terminations is different from the published rates for the normal population. It should be notedthat infliximab does not cross the placenta during the first 10 weeks of pregnancy, at least in rodents. There is insufficient data to advise continuation or starting of anti-TNF therapy, if a patient becomes pregnant. More studies are required to determine infliximab′s safety during pregnancy. Hence, tumor necrosis factor (TNF)-blocking agents, generally should be stopped when pregnancy is discovered. Etanercept:[53] No human data exist, regarding the impact of this drug on human reproductive function. Recently, normal pregnancy and singleton delivery of a healthy infant following chronic (> 1 year) pre-ovulatory TNF alpha-inhibitor therapy for rheumatoid arthritis, has been reported. For this drug also, more studies are required to determine its safety during pregnancy. Hence, it also should be stopped when pregnancyis discovered. IL-1 blocking agents:[53] The safety of IL-1 blocking agents is unknown or has not been established in the pregnancy. There is no data to advise discontinuation of anakinra if a patient becomes pregnant [Table - 3]. Contraception: Combined oral contraceptives are a logical choice because of their effectiveness and possibility that they might improve RA,[33] although contrary reports are available, suggesting that female sex hormones or oral contraceptives do not improve the course of RA.[13],[20] In fact, all reversible methods of contraception are appropriate except intrauterine devices and should not be used in women receiving immunosuppressive therapy.[33] Conclusion In most instances, women with RA can be reassured that successful pregnancy outcome is likely. A majority of them may experience decrease in symptoms and some of them may even go into remission. The remaining patients who are likely to continue with the disease activity, can be effectively managed by adopting the proposed guidelines based on review of literature.References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06050t1.jpg] [ms06050t2.jpg] [ms06050t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}