 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
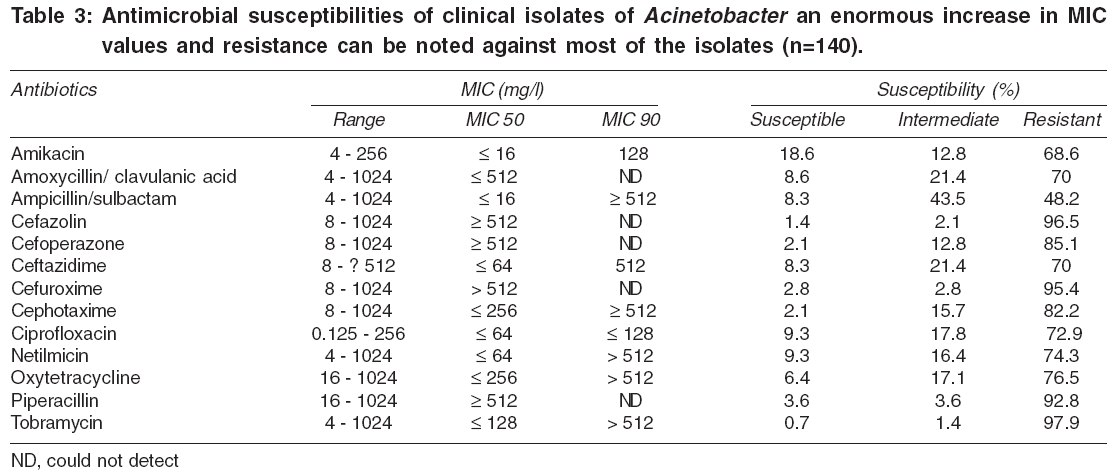
Indian Journal of Medical Sciences, Vol. 60, No. 9, September, 2006, pp. 351-360 ORIGINAL CONTRIBUTIONS Clinical and demographic features of infection caused by Acinetobacter species Joshi SureshG, Litake GeetanjaliM, Satpute MeenakshiG, Telang NilimaV, Ghole VikramS, Niphadkar KrishnaB Department of Clinical Microbiology, King Edward Memorial Hospital, Pune, India Correspondence Address:91, Department of Infectious Diseases, Thomas Jefferson University Medical College, 1020 Locust Street, Room: JAH-314, Philadelphia, PA 19107, USA Email:surejoshi@yahoo.com Code Number: ms06051 Abstract BACKGROUND: Recently, Acinetobacter emerged as an important pathogen and the prevalence of isolation has increased since the last two decades worldwide.AIMS: To determine Acinetobacter incidence, their clinical demography, antibiotyping and speciation. SETTINGS AND DESIGN: A study of the clinical samples submitted to microbiology laboratory of a teaching hospital over a period of 3 years (December 1994 through November 1997). MATERIALS AND METHODS: Identification, speciation and antibiotyping were performed for the isolates of Acinetobacter recovered from infective samples. Clinical demographic characteristics were studied retrospectively. RESULTS: Total 510 of 5391 (9.6%) of isolates were Acinetobacter, responsible for 71.2% (363 of 510) monomicrobial and 28.8% (147 of 510) polymicrobial infections. The organism was responsible for 156 (30.6%) cases of urinary tract infection and 140 (27.5%) cases of wound infection and was most prevalent in the intensive care unit (30.8%, 140 of 455). The crude mortality rate due to multi-drug resistant Acinetobacter septicemia was 7.9% (36 of 455). The isolates could be classified into 7 species, with A. baumannii being most predominant. No peculiar pattern during antibiotyping was observed, but most of them were multi-drug resistant. CONCLUSION: Multi-drug resistant Acinetobacter nosocomial infection has emerged as an increasing problem in intensive care units of the hospital, responsible for 7.9% deaths. The analysis of risk factors and susceptibility pattern will be useful in understanding epidemiology of this organism in a hospital setup. Keywords: Acinetobacter, antimicrobial resistance, hospital-acquired infection, nosocomial pathogen, risk-factor Acinetobacter is ubiquitous, free-living and fairly stable in the environment. Members of the genus Acinetobacter are gram-negative cocco-bacillus that emerge as significant nosocomial pathogens in the hospital setting and are responsible for intermittent outbreaks. The incidence of outbreak is much more in the regions where temperature is hot and humid. The infection caused by Acinetobacter is difficult to control due to multi-drug resistance, which limits therapeutic options in critically ill and debilitating patients especially from intensive care units, where their prevalence is most noted. One of the species, Acinetobacter baumannii , is currently the third commonest isolate from gram-negative sepsis in immunocompromized patients, posing risk for high mortality.[1] The organism prefers moist environment; therefore, colonization in healthy persons and damaged tissue is also common.[2] The infections caused by Acinetobacter usually include pneumonia, septicemia, wound sepsis, urinary tract infection, endocarditis and meningitis.[3] In addition to hospitalized patients, community-acquired Acinetobacter infection is increasingly reported these days.[4] Although epidemiological features and risk factors for outbreaks of Acinetobacter infection have been described, there is a paucity of information about Acinetobacter endemicity. There is a significant difference in behavior of this organism among isolates recovered from various geographic locations.[5] In our study spread over a period of 3 years at a tertiary care teaching hospital; we report the significance of infections caused by Acinetobacter spp. and their biological response towards antibiotic susceptibility patterns. Materials and methods Clinical specimens, bacterial isolates and Acinetobacter identification The study was carried out in a 600-bed tertiary care hospital of Pune, a city from the state of Maharashtra, located in western India, during December 1994 through November 1997. All clinical specimens were initially processed by the routine microbiology laboratory tests to separate the nonfermenters from gram-negative bacilli and eventually identified as acinetobacters.[6] Typical colonies were enumerated, picked and examined further. Acinetobacter was identified by Gram staining, cell and colony morphology, activity in the oxidation / fermentation test, absence of motility and negative oxidase and positive catalase reactions. The transformation assay of Juni was used to confirm the genus.[7] Clinical features of cases of Acinetobacter infection The following clinical characteristics were recorded: Sex, age, seasonal incidence, duration of hospitalization, presence of underlying disease(s) and risk factors, days on previous antibiotic therapy, possible source of infection and clinical outcome of the disease [Table - 1]. The same person retrieved the case records. Standard definitions as given by Center for Disease Control and Prevention were used to differentiate categories of infection and 'infection versus colonization,' etc.[8] All standard precautions were taken to avoid contamination. In brief, the infection acquired upon hospitalization for 72 h or more was hospital-acquired; and it was community-acquired if the patient had not recently been in a health care facility or been in contact with someone who had been recently in a health care facility. Patient from whom Acinetobacter was isolated in absence of clinical disease suggesting colonization were not included in this study. Wherever applicable, to analyze contingency table and statistical significance, GraphPad software program 4.0 for PC (Graph Pad Software, Inc, San Diego, CA) was used, employing Fisher exact test and odds ratio (OD) for relative risk and P value (two-sided). A P≤ 0.05 was considered significant. Method of species identification The genus of Acinetobacter was further speciated into genomic species (Gs) by the method previously published using a battery of series of biochemical tests.[9] Antimicrobial susceptibility testing Antimicrobial susceptibility testing of clinical isolates of Acinetobacter was first performed by the disc-diffusion techniques (Hi-Media Laboratories, Mumbai, India) as described.[10] The MIC of the species was determined according to NCCLS (now Clinical Laboratory Standards Institute, CLSI) guidelines.[11] The following 13 antimicrobial agents were tested: amikacin (30), amoxycillin/clavulanic acid (30, 5:1 ratio), ampicillin/sulbactam (10, 2:1 ratio), cefazolin (30), cefoperazone (75), ceftazidime (30), cefuroxime (30), cephotaxime (30), ciprofloxacin (5), netilmicin (30), oxytetracycline (30), piperacillin (100), tobramycin (10). Figures in parenthesis indicate concentrations in mg used for disk diffusion test. E. coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were included as the control strains for susceptibility testing. Results Features of the cases of Acinetobacter infection During the period of 3 years in clinical microbiology laboratory at the KEM Hospital (affiliated to the University of Pune), Pune (India), 23,009 samples were cultured, of which 23% (5,391) were found infective. Total 510 of 5,391 (9.6%) of the infective samples were Acinetobacter , responsible for either monomicrobial (363) or polymicrobial (147) infection. NNW and ICU samples include all types of clinical specimens collected from the hospitalized patients from locations such as respiratory trap secretions, sputa, blood, urine, wound exudates, intravenous catheters and tips, stool, cerebrospinal fluid (CSF), other body fluids as indicated. The variables such as age, sex, seasonal incidence, hospital-versus community- acquired infection, possible source of infection and risk factor distribution analyzed are shown in [Table - 1]. Total number of cases from which percentage is derived is also shown for respective variables. The highest incidence was noted during the months of April-May and October, while the lowest in January (data not shown). The male and female cases are the total, which include ICU and various wards. Similarly, the duration of hospital stay is also applicable to the patients from ICU, NNW and other wards such as medical, surgical, trauma and burns. The source of infection indicates the obvious and confirmed sources and all other doubtful and nonconfirmed sources are classified here as unknown sources. In some of the bacteremia cases, although Acinetobacter was isolated, the primary source of infection could not be tracked and therefore was categorized under unknown source of infection [Table - 1]. About 2.2% (11 of 510) of bacteremia cases confirmed were due to intravenous catheters, as evident from cultures of tips. Among the sources or sites of infection, pus and wound exudates were extremely significant (OD, 0.7063; P < 0.0001), followed by urinary tract (OD, 1.348; P < 0.0071) and respiratory tract (OD, 0.2114; P < 0.0001). Likewise, the risk factor distribution associated with various clinical wards/units are also shown in [Table - 1]. Acinetobacter infection was significantly observed in neonatal care unit (OD, 0.1859; P < 0.0001) and intensive care unit (OD, 0.7329; P < 0.0079). The sole cause of death shown is multi-drug resistant (MDR) Acinetobacter septicemia, as indicated in case records by clinician′s remarks. The number of deaths indicates a crude mortality rate. It appears from [Table - 1] that during second week of hospitalization, Acinetobacter infection was remarkably high (34.5%, 157 of 455; P < 0.001). The infective urine samples (30.6%) are mainly the ICU urinary tract infection cases. Existing chronic debilitating diseases or conditions mainly include chronic obstructive pulmonary disease, end-stage renal disease, diabetes mellitus, malignancies, hepatic or chronic cardiac failure as defined earlier.[12] A detailed case analysis is not shown and found beyond the scope of the present report. Speciation of Acinetobacter Species differentiation of the isolates and their distribution in clinical specimens is shown in [Table - 2]. It is observed from the analyses that genomic species (Gs-2) ( A. baumannii ) is a predominant species responsible for 70% of the infection, followed by Gs-5 ( A. junii ) and Gs-3 (8.6 and 7.2% respectively). Urine and wound exudates were significant contributors towards infection with A. baumannii . Two samples of CSF were found positive for A. calcoaceticus (Gs-1), collected from the cases of neonatal meningitis, in addition to A. baumannii and Gs-11. One isolate of A. johnsonii (Gs-7) was recovered from peritoneal fluid, whereas A. hemolyticus (Gs-4) was predominantly found in wound exudates. Antimicrobial susceptibilities of acinetobacters The results of antimicrobial susceptibilities against acinetobacters are presented in [Table - 3]. Majority of the isolates were multi-drug resistant, showing resistance to two or more antimicrobial agents. MIC for most isolates against majority of antimicrobials was very high [Table - 3]. The percentage of resistant isolates against third-generation cephalosporins and β -lactam plus β-lactamase inhibitor is found rising over years as compared to earlier reports.[13] Tobramycin - once upon, one of the drugs of choice for pediatric patients - showed loss of its efficacy against MDR Acinetobacter isolates. The isolates were fairly susceptible to amikacin, though less than ampicillin/ sulbactam [Table - 3]. All MICs were found highly elevated in these isolates, demonstrating a rising concern for infection control in hospitals. The higher resistance was observed in urinary and ICU isolates (data not shown) where A. baumannii was most prevalent. Discussion Acinetobacter is an important nosocomial pathogen, with a rising prevalence of hospital-acquired infection.[2],[13],[14] About 89.2% of Acinetobacter recovered were from hospitalized patients, whereas only 10.8% from community-acquired OPD cases. Hospitalized patients (wherever n=455) were mostly included for risk factor assessment, whereas for some of the categories of demographic features such as sites of infection and information of previous antibiotic therapy (wherever n=510), total number of indoor and outdoor cases were considered. It depended upon the net and confirmed information available. The overall incidence of Acinetobacter isolation from all infective samples was 9.5% (510 of 5391), indicating its importance as a nosocomial pathogen, since in most cases the patients were symptomatic for sepsis. A slightly higher incidence in males than females is comparable to other reports from Indian studies[15] and do not have statistical significance. A high (April-May and October) or low (January) seasonal incidence in Acinetobacter infection may be correlated with atmospheric temperature changes (data not shown) and is found comparable to earlier reports.[16] The literature search demonstrates that genomic species Gs-2 ( A. baumannii ), together with Gs-1 ( A. calcoaceticus ), Gs-3 and Gs-13TU, is predominantly involved in infection and is often collectively known as the Acinetobacter calcoaceticus-A. baumannii ( Acb ) - complex.[17] This holds true in our study too. About 79% of the isolates belonged to Acb - complex group. A. baumannii , a major species isolated from most of the clinical specimens of this hospital, is reportedly a main species responsible for nosocomial infection in other parts of the world also.[5] A. johnsonii (Gs-7) was also isolated from ascitic fluid and has not been reported so far as a cause of infection of peritoneum, although bloodstream infection is reported. Isolation rate from blood in this study at 7% (70 of 510) was comparable to earlier reports from some of the countries such as France and Belgium but much less than in reports from USA and Germany.[2] Although bacteremia is known to be associated with risk factors of invasive procedures such as intravenous catheterization,[18] many a times source/site of infection is of unknown origin.[19] In this study, about 2.2% of bacteremia cases were associated with intravenous catheterization. Total isolates from all urine samples (including ICU and NNW) were 30.6%, which is less than some of the reports but comparable to reports from USA and Belgium.[2] The strains showing multi-drug resistance were highest from the urinary isolates (mainly because of A. baumannii, which were resistant). In our study, the significant risk factors for Acinetobacter infection were a previous ICU stay and prior exposure to third-generation cephalosporins. The identification of ICU as a strong risk factor is not unexpected. A longer stay in a high-risk unit has been identified as a risk factor in previous studies.[15],[16],[17],[18],[19],[20] In our studies, a hospital stay of about 8 to 14 days was a major risk factor. A hospital stay of more than a week and prior use of broad-spectrum antibiotics or fluoroquinolones were significant risk factors for Acinetobacter in other studies.[21],[22] Our observation demonstrates that insufficient previous antimicrobial therapy is one of the high-risk factors in Acinetobacter nosocomial infection. There are few studies analyzing risk factors for the acquisition of multi-drug resistant Acinetobacter .[15],[22],[23] In our study, the significant risk factors for Acinetobacter infection were not only a previous ICU stay and prior exposure to third-generation cephalosporins, but also variables related to hospitalization and invasive procedures such as indewelling catheters, intubation and catheter lines. An association between cephalosporins and Acinetobacter infection has been reported earlier.[24] The role of exposure to certain antibiotics provides a selective advantage to a small number of resistant organisms in patients already colonized, thereby enabling them to turn into pathogens at the earliest opportunity. In many patients, Acinetobacter spp. showing two different antibiograms were isolated from different clinical specimens of the same individual, alarming for the necessity for clinically correlating the isolate as a pathogen or commensal.[2],[22] Despite many intensive efforts, the nosocomial acquisition of Acinetobacter remains problematic, especially in ICUs. Molecular epidemiologic studies have revealed the presence of heterogenous strains in a given hospital or service center where they have become both endemic and epidemic,[25] especially the members of Acb - complex.[17] There are difficulties both in control and nosocomial infection due to their high resistance to antimicrobials in hospital environment. Susceptibilities to Acinetobacter spp. against antimicrobials is considerably different among countries, centers and even among the wards of a given hospitals and therefore such type of local surveillance studies are found important in deciding the most adequate therapy for Acinetobacter infections. The development of resistance to antimicrobials in Acinetobacter appears to be unstoppable, when we compare the study reports published over time.[3],[13],[14],[15],[26],[27] Also, there are very few reports showing studies conducted on synergy between the latest β -lactams, β -lactamase inhibitors and an aminoglycoside,[28] a need especially for polymicrobial or mixed nosocomial infection. In our study, the overall range of MICs is much higher than recent reports.[27] The MICs of ampicillin/sulbactam, plus amikacin, also seem to be rising enormously, showing about 48.2 and 68.6% resistance respectively [Table - 3] for the drugs that were once the treatment of choice. These figures are comparable but slightly higher than many other reports.[3],[13],[27],[18] This also means MDR isolates of Acinetobacter are increasing day by day and this is one of the reasons for rapid spread of resistance. We could not perform susceptibility testing for carbapenems such as imipenem, meropenem and monobactams as these were not available from the local suppliers during this study. Colistin, bacitracin and polymyxin B, when tested by disk diffusion testing, showed resistance in 62.8, 92.9 and 61.2% of the isolates, but MICs could not be carried out due to non-availability from suppliers (data not shown). Nevertheless, the percentage of resistance to these antimicrobials appeared to be risen. Polymyxin B and colistin have demonstrated a reasonable success in control of MDR Acinetobacter in the past, but for selected cases of serious nature due to their higher toxicities. Furthermore, there are pharmacodynamic issues still needed to determine appropriate dosage regimens that will optimize effectiveness and minimize toxicity.[29] Possible colistin resistance in about 62.8% isolates (as mentioned above) also reflects a rise of colistin-resistant strains, which may create an alarming clinical situation. Transferable antimicrobial resistance has also been reported in our hospital,[30],[31] which very few study groups have reported from elsewhere. Reducing sensitivities to amikacin, netilmicin and co-amoxyclav have been reported by Tankovic et al,[32] showing the higher potential of this genus to develop antibiotic resistance leading to multi-resistant isolates in environments, especially hospital setups. Conclusion Acinetobacter is emerging as multi-drug resistant nosocomial pathogen, increasingly involved in hospital-acquired infections. Its prevalence is much more in ICU, where the selective pressure of antibiotics is already high, showing a need for rational use of antimicrobials. Strict infection-control measures may prevent nosocomial infection and reduce mortality. Risk factor analyses will be useful for further hospital epidemiology studies of Acinetobacter . Further research related to mechanisms of resistance and extended-spectrum beta-lactamase patterns and current carbopenem and monobactam is underway. Acknowledgment A part of the data was presented to the University of Pune. There is no conflict of any degree of commercial or potential dual interest.References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06051t2.jpg] [ms06051t1.jpg] [ms06051t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}