 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
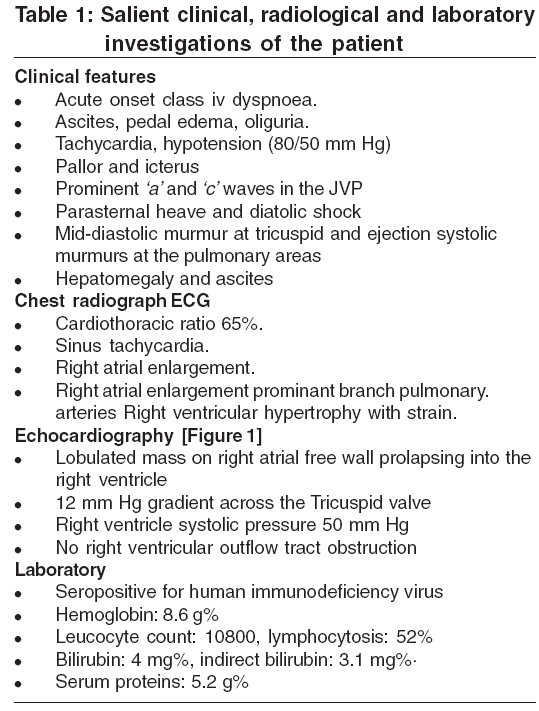
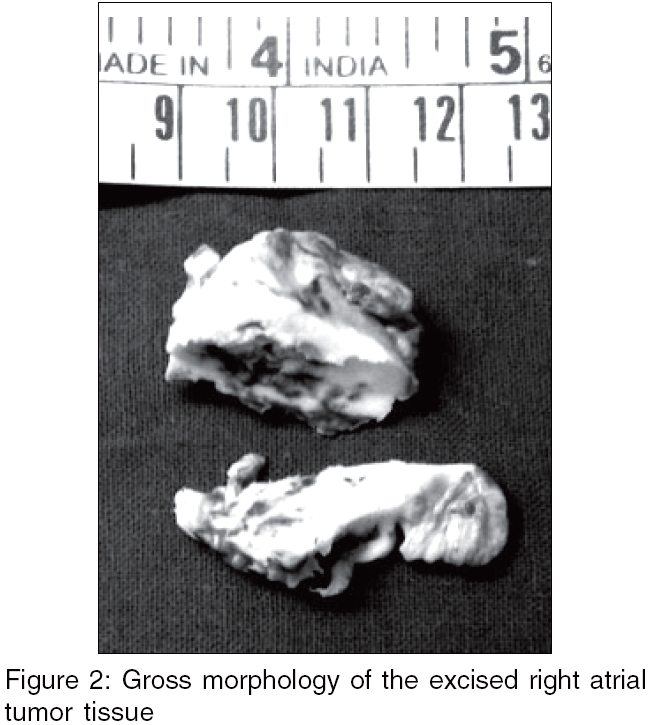
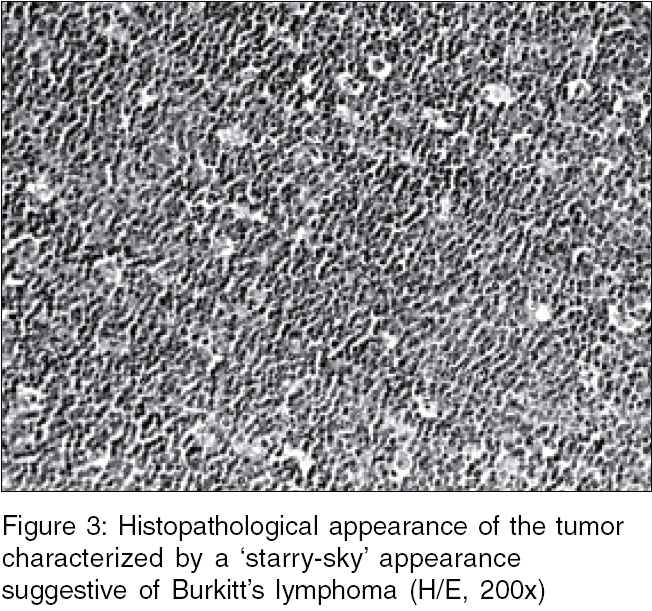
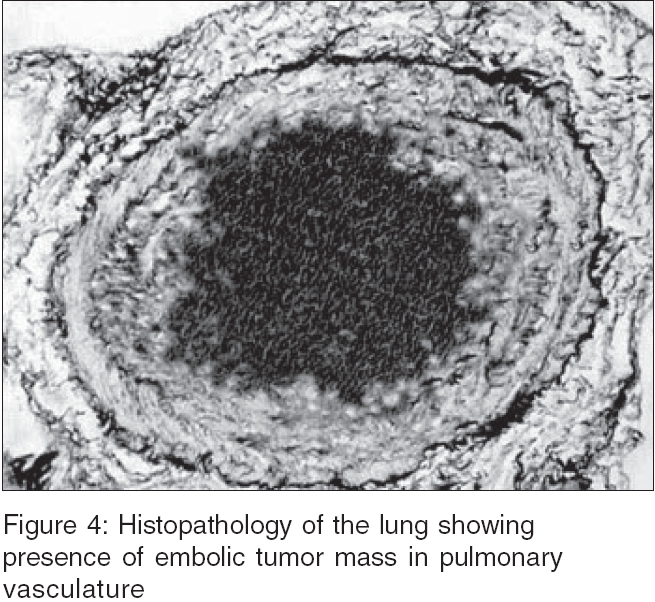
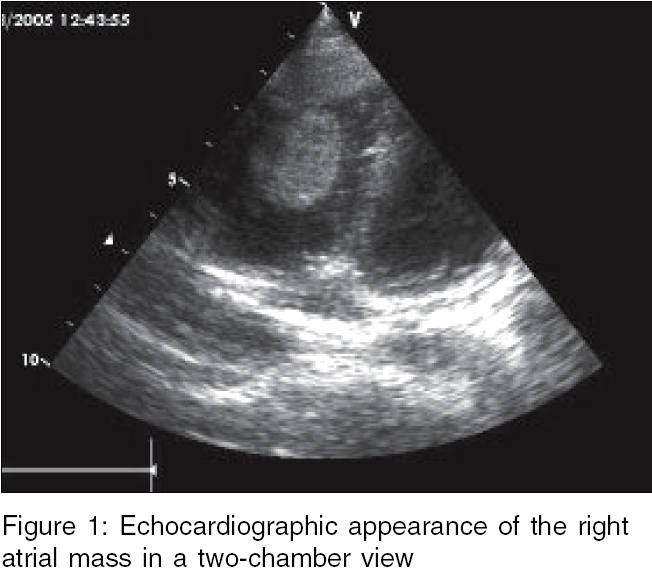
Indian Journal of Medical Sciences, Vol. 60, No. 9, September, 2006, pp. 380-384 Case Report Fatal secondary pulmonary hypertension due to cardiac involvement in AIDS-associated Burkitt's lymphoma Singh AshutoshS, Dave DhirenJ, Thanvi Sunil, Atre DhanashriA, Parikh Prashant, Patel NehalH U. N. Mehta Cardiology Institute, Ahmedabad, Gujarat Correspondence Address:International Centre of Cardiothoracic and Vascular Diseases, Frontier Lifeline Hospital, Chennai - 600 101 Email: dhirendave2002@yahoo.com Code Number: ms06055 Abstract Primary cardiac lymphomas are rare lesions in children with acquired immunodeficiency syndrome (AIDS). Most of them are high-grade Burkitt's or Burkitt-like lymphomas. They usually present with congestive cardiac failure, pericardial effusion or tamponade, arrhythmias, with predominant systemic 'B' symptoms and often with widespread extranodal involvement. The clinical profile and operative and pathological findings of a 4-year-old boy with AIDS-associated Burkitt's lymphoma of the heart presenting with acute right heart failure and fatal secondary pulmonary hypertension is reported.Keywords: AIDS-associated Burkitt′s lymphoma, cardiac lymphoma, pulmonary hypertension Introduction Though the prevalence of malignant lymphomas in acquired immunodeficiency syndrome (AIDS) is 20-60 times more than in general population, involvement of the heart is infrequent, reported mostly as individual cases.[1],[2] Majority of these AIDS-associated lymphomas are high-grade Burkitt's or Burkitt-like lymphomas.[3] The unusual clinical presentation of AIDS-associated Burkitt's lymphoma in a 4-year-old boy seropositive for human immunodeficiency virus (HIV) as acute right heart failure due to right ventricular inflow obstruction followed by fatal secondary pulmonary hypertension due to chronic embolisation is reported here.Case report A 4-year-old boy presented to us with worsening acute onset dyspnea, NYHA class IV orthopnea, oliguria, pedal edema and abdominal distension. There was no history suggesting rheumatic fever or other preceding illnesses. The clinical, radiological and investigation profile is summarized in [Table - 1]. The child was taken up for an emergency surgical excision of the right atrial mass. The pericardium was not involved and there was no pericardial effusion. The surgery was performed via a median sternotomy and standard cardiopulmonary bypass was instituted by aorto-bicaval canulation on moderate hypothermia. Myocardial protection was achieved by electromechanical arrest with antegrade cold blood potassium cardioplegia after clamping the ascending aorta. The pulmonary artery was vented. After caval snaring, the right atrium was opened longitudinally parallel to the atrioventricular groove. There was a single lobulated friable mass attached to the free wall of the right atrium. The tricuspid valve was free of the tumor. The mass was excised with a rim of right atrial wall. There was no other tumor in the heart. The atriotomy was closed and the patient was weaned of cardiopulmonary bypass. A pulmonary arterial catheter was placed for monitoring. There was no involvement of the mediastinal lymph nodes. The lungs were unremarkable on gross appearance. The child was shifted to the ICU with stable hemodynamics on inotropic supports. Postoperatively, the patient persistently had high pulmonary artery pressures. His arterial blood gases showed a gradual development of hypoxia, hypercarbia and acidosis. He deteriorated on the third postoperative day and expired. Grossly, the tumor has a lobulated grayish white appearance [Figure - 2]. There were areas of necrosis and hemorrhage on cross section. On histopathology [Figure - 3], the tumor was found to be composed of monomorphic, medium-sized cell-large round nuclei; multiple nucleoli; and abundant basophilic cytoplasm. There were numerous benign macrophages scattered throughout the section, giving a 'starry-sky' appearance typical of Burkitt's lymphoma. Cross section of lung specimen showed diffuse distribution of tumor emboli throughout the parenchyma. Lung biopsy confirmed presence of Burkitt's tumor in the pulmonary vasculature [Figure - 4]. Discussion Malignant lymphomas constitute the primary manifestation of AIDS only in 3-4% of the population.[1] Primary cardiac lymphoma is a very rare malignancy, accounting for about 1% of the primary cardiac tumors and 0.5% of the extranodal lymphomas. However, disseminated lymphoma with cardiac involvement can occur in up to 20% of patients.[4] Most non-Hodgkin′s lymphomas affecting the heart in HIV infection are high grade, with Burkitt-like cells, reticular cell sarcomas or large cell immunoblastic sarcomas, collectively termed as AIDS-associated Burkitt′s lymphomas. The majority originate from B cells.[1],[2] Cardiac lymphomas usually demonstrate pallor of the heart secondary to diffuse lymphomatous infiltration or patchy involvement of the epicardium, myocardium and endocardium in the form of focal circumscribed nodules, most frequently affecting the right atrium.[5] The tumor in this case was a right atrial mass lesion attached to its free wall, an uncommon finding. AIDS-associated cardiac lymphomas present clinically as congestive cardiac failure, pericardial effusion or tamponade, arrhythmias.[6] Predominance of systemic ′B′ symptoms like fever, drenching night sweats and weight loss in excess of 10% of normal body weight are described in as many as 82% of patients with systemic AIDS-associated lymphomas. These patients often present with widespread extranodal involvement; it was found to be occurring in 88 of 90 (98%) patients included in a large, multi-center retrospective report.[7],[8] The patient mentioned here had neither of these and had presented initially as acute right heart failure due to right ventricular inflow obstruction by right atrial mass lesion. The excision of the tumor however did not restore the hemodynamics to normal. The pulmonary artery pressures remained high postoperatively and the child succumbed to right heart failure. Autopsy findings suggested chronic embolisation of the lung vasculature by lymphomatous tissue. The involvement of any extracardiopulmonary system was remarkably absent. Primary pulmonary hypertension affects about 0.5% of hospitalized adults with AIDS and is a cause of severe cardiac impairment with associated cor pulmonale and death.[9] Right heart tumors are known to embolise to lungs and lead to secondary pulmonary hypertension.[10] Fatal secondary pulmonary hypertension caused by AIDS-associated Burkitt's lymphoma in a child with AIDS has not been described previously to the best of our knowledge. Detailed histopathological and immunohistochemical studies were not done in view of its normal gross features. This remains a major limitation of this report. Outcome is usually poor in these patients and the optimal approach to treatment has yet to be determined. Clinical remission has been obtained with combination chemotherapy with highly active antiretroviral therapy. Ratner et al.[11] in their series of 65 patients have shown that both modified and full-dose regimens of cyclophosphamide and doxorubicin, combined with vincristine and prednisone, with highly active antiretroviral therapy are effective and well tolerated in patients with HIV-associated non-Hodgkin's lymphomas. Though chemotherapy has been the mainstay of treatment in these patients, the case discussed here had to undergo emergency cardiac surgery in view of his worsening hemodynamics. Secondary pulmonary hypertension leading to fatal right heart failure can be a clinical presentation of AIDS-associated Burkitt's lymphoma in children with AIDS. A high index of suspicion and optimum chemotherapy regimen with highly active antiretroviral therapy may help in improving the outcome of this potentially lethal condition. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06055f2.jpg] [ms06055f1.jpg] [ms06055f4.jpg] [ms06055f3.jpg] [ms06055t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}