 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
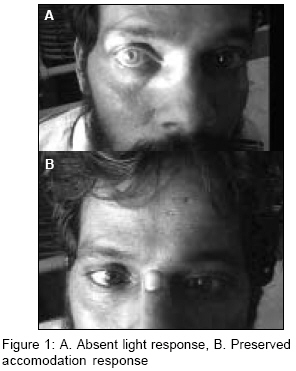
Indian Journal of Medical Sciences, Vol. 60, No. 10, October, 2006, pp. 421-422 Letter To Editor Syphilitic myeloradiculopathy and pupillary light near disassociation: An overlap syndrome in a HIV positive individual Raji V, Dhanasegaran SE, Subramanian K, Sivaprakash S Institute of Internal Medicine, Madras Medical College, Chennai Code Number: ms06062 Sir, 35 years old male was admitted for unsteady gait and bladder incontinence of 20 days duration. He gave a history of premarital heterosexual exposure fifteen years back following which he developed penile ulcers. Neurological examination revealed right sided foot drop with 4/5 power in knee and hip bilaterally. He had absent ankle reflexes with an extensor plantar response on right. He had diminished sense of vibration and joint position sense over the lower extremities. Romberg′s test was positive. The right pupil was dilated and did not react to light but reacted briskly to accommodation (Light-Near disassociation-LND) [Figure - 1]A, B. He had dribbling incontinence with absent anal reflex and perianal sensory loss. The complete haemogram, renal functions, liver functions, Chest X-ray, ECG, Vitamin B12 levels, were normal. His ESR was 40 mm/hr. His blood VDRL was reactive in 1 in 64 dilutions. His Cerebrospinal fluid (CSF) analysis revealed an elevated protein (60 mg%), low sugar (15 mg%) and 8-10 lymphocytes. CSF VDRL was reactive in 1 in 8 dilutions. CSF TPHA (treponema pallidum hemeagglutination assay) was positive. CSF gram stain, India ink stain and AFB stain were negative. He also tested positive for HIV antibodies and his CD4 count was 529 cells. MR imaging of the spinal cord and the brain was normal. Nerve conduction studies in both the lower limbs tibial, common peroneal, sural nerves were abnormal suggestive of polyradiculopathy. Patient was started on steroids for the myeloradiculopathy pending the CSF reports. Patient was later started on benzyl penicillin (12 lakhs IU intramuscular) for 21 days. The patient regained normal power and sensations in both lower limbs and bladder control. The pupillary abnormality (LND) persisted. Patient was discharged and was advised follow up at monthly intervals. The neurological manifestation of syphilis were earlier classified as general paralysis of insane, Tabes dorsalis and Meningovascular syphilis. The manifestations of meningovascular syphilis varied from the "pure" basal meningitis form (hydrocephalus, cranial nerve palsies) to "pure" vascular form with rarer presentation of spinal cord involvement in the form of Erb′s spastic paraplegia, Syphilitic acute and chronic myelitis, Pachymeningitis hypertrophica cervicalis, Syphilitic amyotrophy. However in this era of advanced neuroimaging and electrophysiological studies the relevance of these terms and disease labels remain questionable. A recent study by Timmermans et al has shown that there could be a considerable overlap in the manifestations of neurosyphilis, particularly with a HIV-syphilis coinfection. The study group divided neurosyphilis into six syndromic categories.[1] They include the neuropsychiatric, cerebrovascular, ocular, myelopathy, seizure, brain stem involvement. HIV infection may increase the frequency or accelerate the development of neurological sequelae of syphilis.[2] Thus the clinically based classification will help us accommodate various manifestations and create a standard nomenclature for case reporting. Our case would be an overlap of myeloradiculopathy and brainstem involvement. HIV co-infection also leads to higher rate of serological failure and relapse.[3],[4] Thus the mainstay in treatment is vigilant monitoring of therapeutic response at 3 monthly intervals for 12-24 months. Acknowledgement Dr. Natarajan V, MD, DM Professor of Neurology, Madras Institute of Neurology, Chennai.References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06062f1.jpg] |
| |||||||||

{kind=link}