 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 60, No. 11, November, 2006, pp. 454-460 Original Contributions Evaluation of outcome of various treatment methods for endogenous endophthalmitis TULSI KESWANI, VIJAY AHUJA*, MANISH CHANGULANI** National Institute of Ophthalmology, Pune, *Bombay Hospital,
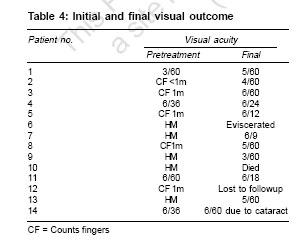
Indore, **King George Medical College, Lucknow, India Code Number: ms06067 Abstract AIM: To evaluate the role of different treatment methods (intravitreal antibiotics and vitrectomy) for endogenous endophthalmitis and assess the outcome. Keywords: Endogenous, endophthalmitis, intravitreal antibiotics, vitrectomy Endogenous endophthalmitis is a potentially blinding intraocular infection resulting from the hematogenous spread of organisms from a distant source of infection (e.g., endocarditis). It is relatively rare, accounting for 2-8% of all cases of endophthalmitis and is associated with immunocompromised state, debilitating diseases and invasive procedures.[1] Due to the rapid advance of medical technology, a longer lifespan of patients with chronic disease and a rising prevalence of long-term intravenous access, the disease may become more common in clinical practice. Many etiological organisms (gram-positive, gram-negative and fungal) have been reported to cause endogenous endophthalmitis.[2],[3] A high clinical suspicion is needed for early diagnosis and treatment. A classification system introduced by Greenwald[4] takes into consideration the affected areas of the globe and the associated visual prognosis. Focal endophthalmitis responds well to intravenous antibiotics and generally results in minimal sequelae. Posterior diffuse endophthalmitis and panophthalmitis are associated with a much poorer prognosis; often these conditions lead to blindness, atrophy of the globe or enucleation. Early intravenous antibiotic therapy remains the cornerstone of treatment.[4] The role of intravitreal antibiotics and vitrectomy is evolving and they may become more widely accepted as therapeutic modalities. It is important that a general practitioner is aware of endogenous endophthalmitis because early diagnosis and prompt aggressive treatment are imperative if vision loss is to be avoided. The objective of this study was to evaluate the role of intravitreal antibiotics and vitrectomy in improving final visual outcome in patients with endogenous endophthalmitis. Materials and methods This is a retrospective observational case study conducted at a hospital in Visakhapatnam, India. Fourteen patients of endogenous endophthalmitis seen between October 2000 and April 2004 were reviewed. Patients were considered to have endogenous endophthalmitis if at least one of the following three criteria were met: a. Growth present on more than one media from vitreous or aqueous cultures b. A positive blood culture result c. Posterior and/or anterior ocular inflammation All patients underwent detailed clinical ocular examinations (visual acuity by Snellen chart, slit lamp biomicroscopy and indirect ophthalmoscopy). All patients were also seen by the concerned physician to find out the source of infection. All diagnostic tests, chest X-ray, CT scan of orbit, cardiac ultrasound and echocardiography were done, which were helpful to find out the focus of infection. The culture and sensitivity of non-ocular sites like blood and urine were done. Blood culture was done thrice in all cases.[5] Aqueous and vitreous cultures were also done whenever possible by an ophthalmic surgeon; sterile needles were used to aspirate material. Because of the small amounts of material involved, inoculation of plates and preparation of slides were done at the patient's side. The initial vitreous aspirates were sent for smear, culture (bacterial and fungus) and antibacterial sensitivity. These samples were subjected to Gram stain, Periodic Acid Schiff stain and calcofluor stains for direct microscopy under light and fluorescent microscope and cultured on 5% blood and chocolate agar (any organism), anaerobic thioglycollate broth and Sabourauds agar media (fungi).[6] A standard clinical pro forma was used for all cases for analytic study, which included age, sex, clinical findings, ancillary test and anatomical type of endophthalmitis. The results were analyzed using descriptive statistics and frequency analysis. Results Fourteen patients of endogenous endophthalmitis were analyzed in this study. Eight (57%) of the 14 patients were males and 6 (43%) were females [Table - 1]. Average age at time of presentation was 61 years with a range of 20 to 75 years. Five patients belonged to the age group of 60-70 years, 5 to 41-60 years, 3 to 21-40 years and only 1 patient to 0-20 years. Out of the 14 patients, 12 patients had unilateral involvement (5 right eyes and 7 left eyes were in the current series) and 2 patients had bilateral involvement. All patients had history of other systemic illnesses. Of these 14 patients, 6 had diabetes, 3 had CRF, 1 had chest infection, 2 had UTI, 2 were on immunosuppressive drugs, 1 had endocarditis, 1 had hepatitis, 1 had abdominal surgery, 1 had head injury and 1 had meningitis. Patients were referred to us or came directly at varying periods - between 1 and 14 days - after the onset of symptoms. Out of 14 patients, 9 were already admitted in acute medical care and 5 came directly to ophthalmology outpatient department. Examination findings were recorded [Table - 2]. Eight (50%) out of 16 patients presented with focal posterior endophthalmitis, 4 (25%) with diffuse posterior endophthalmitis and 4 (25%) with combined (anterior and posterior) diffuse endophthalmitis. Four (25%) patients had hypopyon in addition to vitreous exudates. Out of 14 patients, only 1 (7%) patient had positive blood culture, 2 (14%) had positive urine culture, 1 (7%) had positive wound culture, 1 (7%) had CSF culture positive and one (7%) patient had positive culture on catheter tip [Table - 3]. Out of 16 eyes, 12 (75%) eyes were treated with intravitreal (vancomycin-amikacin) and intravenous antibiotics (vancomycin + ceftazidime) and 4 (25%) patients were managed by intravenous antibiotics only (vancomycin-ceftazidime) [Table - 2]. Out of these 12 patients, who were treated with intravitreal antibiotics, 8 (66%) were culture-positive (intravitreal) and the rest 4 (33%) were culture-negative. Out of the 8 patients who were culture positive, 4 were positive for fungus (3, candida; 1, aspergillus), 2 for gram-positive (1, S. aureus; 1, Streptococcus pneumoniae) and the remaining 2 for gram negative (1, Pseudomonas; 1, Klebsiella). Anterior chamber tap was done for (4 eyes) hypopyon for anterior chamber cleaning as well as for therapeutic purposes and was sent for microbiology. Three cases were culture-positive (2 for fungus, 1 for gram-negative) and 1 was culture-negative. Out of the 4 patients who were found to have fungal endophthalmitis, 3 patients underwent pars plana vitrectomy with injection of amphotericin B. One patient died due to septicemia. All 14 patients (16 eyes) presented with visual acuity from hand movement to 6/36 [Table - 4]. Final visual outcomes were obtainable for 13 eyes (1 patient died due to septicemia, 1 patient was lost to follow-up and 1 eye was eviscerated). Overall, 5 (38%) of 13 patients had final visual acuity of 6/60 or better (1 - 6/24, 1 - 6/18, 2 - 6/12 and 1 - 6/9); the rest (8 eyes - 62%) had visual acuity of less than 6/60 (CF 1 m to 6/60). It was observed that bacterial infection had better outcome as compared to fungal endophthalmitis.[7],[8] Discussion Metastatic endophthalmitis is a rare entity, which occurs at an average annual incidence of about 5 in 100,000 hospitalized patients. It can occur at any age, ranging from 1 week to 85 years. Bilateral involvement is seen in 14 to 25% of patients and reports have shown a higher incidence of involvement of right eye versus left eye[3] in patients with unilateral disease. There is no sex preponderance. Once the diagnosis has been made or strongly considered, prompt consultation with an ophthalmologist is needed. Treatment depends on the underlying cause of endophthalmitis. Final visual outcome is heavily dependent on timely recognition and treatment. Once the diagnosis of candidial endophthalmitis is made, admit the patient to the hospital, start intravenous or intravitreal amphotericin B and oral fluconazole. The prognosis is extremely variable because of the variety of organisms involved. The visual acuity at the time of diagnosis and the causative agent are most predictive of outcome. The outcome of endogenous endophthalmitis is generally worse than exogenous endophthalmitis due to the profile of the organisms typically involved with this form (i.e., more virulent organisms, compromised host, delay in diagnosis). The prognosis appears to also be related to the patient's underlying health conditions, with one study demonstrating worsened outcomes among diabetic patients.[8] Prompt administration of intravenous antibiotic therapy plays a key role in the acute management of endogenous endophthalmitis.[7] Several studies are investigating new molecules with better antibacterial activity and less ocular toxicity. Until these results are available, the evaluation and therapeutic choice remain the surgeon's best judgment. In our study, we found 9 cases of endophthalmitis in the total acute medical care department (around 6,000 patients in 3 years). We found a higher incidence in advanced age group (10 cases out of 14 in the 'more than 40 years old' age group), bilateral involvement in 2 patients (out of 14) - 13%. We did not find much difference between incidences in the right and left eye. The majority of patients have associated predisposing conditions. Several studies have shown diabetes mellitus to be the most common association. (In one series, it was in the range 80-90%). We also found endophthalmitis in 6 (42%) diabetic patients out of 14. In different published series, fungal organisms account for more than half of the cases of endogenous endophthalmitis in which candida albicans is the most frequent cause (75-80%) and in our study fungal organism was found in 4 cases out of 8 culture-positive cases, in which 3 (75%) cases were of candida.[5] Debate exists over the intraocular aspiration / biopsy of endogenous endophthalmitis. Blood, urine, cerebrospinal fluid, complete blood count with differential (evaluating for signs of infection, elevated white count), (erythrocyte sedimentation rate (evaluating for rheumatic causes, chronic infections or malignancy), blood urea nitrogen (evaluating for renal failure or patients at increased risk), wound culture and smear may be indicated to locate the original infection and document systemic involvement. In one study, vitreous showed the highest yield (74%), followed by blood culture (72%).[9] In our study also, non-ocular culture was positive in 6 cases out of 14 (42%); however, ocular culture was positive in 8 cases out of 12 (66%). Role of intravitreal antibiotic injections and vitrectomy has been debated, but recent reports suggested that cases of marked intraocular infection (vitritis preventing visibility of optic nerve head or macula) should be managed similarly to cases of acute postoperative infectious endophthalmitis. In our study, 12 eyes were given intravitreal antibiotics and subsequently all eyes with fungal endophthalmitis (3 eyes) underwent vitrectomy with injection of amphotericin B. In our study, we found that there was a definite improvement in ocular signs and visual acuity after vitrectomy and intra-vitreal injection of antibiotics. Conclusion Our experience suggests that endogenous endophthalmitis is generally associated with poor visual outcome. Prompt treatment with intravitreal antibiotics and vitrectomy can result in improvement in ocular signs and visual acuity in majority of the patients. Patients with culture-positive endogenous endophthalmitis are more likely to have fungal isolates with a predominance of candida. Fungal endopthalmitis may be associated with a poor visual outcome as compared to bacterial endophthalmitis; however, this claim needs to be substantiated with further studies. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06067t1.jpg] [ms06067t4.jpg] [ms06067t2.jpg] [ms06067t3.jpg] |
| |||||||||

{kind=link}