 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
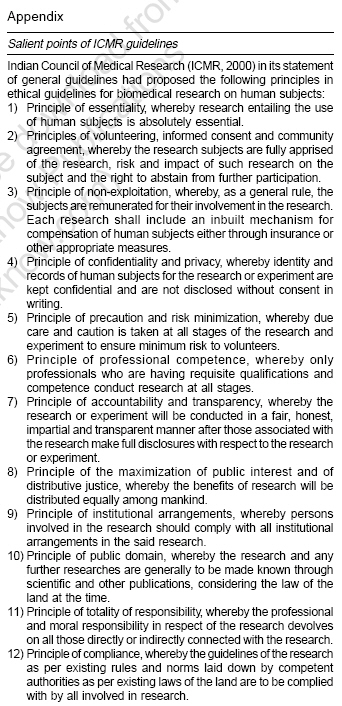
Indian Journal of Medical Sciences, Vol. 60, No. 11, November, 2006, pp. 475-484 Practitioners section Ethical problems faced in villages of rural bengal while conducting researches on chronic diseases like diabetes Mitra Analava, Bhattacharya D SMO, B.C. Roy Technology Hospital, Indian Institute of Technology, Kharagpur, West Bengal - 721 302, and Adjunct Faculty School of Medical Science and Technology, Indian Institute of Technology, Kharagpur - 721 302 Code Number: ms06072 Abstract India is facing an explosion of diabetes and related diseases. Health infrastructure in rural India is very poor. A large number of rural Indians are below poverty line. To overcome the problem of insulin resistance in rural India, the authors conducted studies with nutraceuticals and came across many sociocultural, socio-political and socioeconomic constraints to faithfully following ethical guidelines of Indian Council of Medical Research (ICMR). This paper deals with some of the constraints and it is strongly felt that the ICMR should review its guidelines in the context of the existing situation. Keywords: Diabetes, guidelines, Indian Council of Medical Research, nutraceuticals, rural A researcher, especially one conducting survey-oriented work particularly involving economically backward rural population of the country, comes face to face with some ethical problems vis-à-vis the general guidelines proposed by the Indian Council of Medical Research.[1] The present work describes the authors' experience while carrying on with their work on the studies on effects of nutraceuticals in controlling type 2 diabetes diagnosed at an initial stage as a part of diabetes control and diabetes care program in rural sectors. It necessitated willing long-term participation of the subjects complying with regularly taking food as instructed by the researchers and suggests the necessity of modifications in the guidelines, based on the ground realities. The disease pattern in India is changing rapidly and incidence of chronic diseases like insulin resistance syndrome (manifested by obesity, hypertension, dyslipidemia, atherosclerosis and type 2 diabetes) is increasing by leaps and bounds and assuming an alarming proportion. The authors surveyed parts of West Midnapore district in West Bengal to ascertain the effects of different nutraceuticals on containing the incidence of insulin resistance syndrome. Hence the main objective of the work was to devise a diabetic care program. Difficulties encountered Problem of language 1) Informed consents of the subjects or their legal guardian were taken, respecting their autonomy and freedom. The subjects were given all information regarding the study and all their relevant questions were answered in order to clear up their doubts ( vide Indian Council of Medical Research (ICMR) general guidelines of principle of essentiality and principles of volunteering, informed consent and community agreement. ICMR, in general guidelines item 1, states the principle of essentiality as situations whereby the research entailing the use of human subject is absolutely essential. ICMR, in item 2, state the principles of volunteering, informed consent and community agreement, whereby the research subjects are fully apprised of the research, risk and impact of such research on the subject and the right to abstain from further participation). 2) Witnesses in the process of informed consent so taken were preferably not related to the subject. The subjects were informed in their own dialect. Not only is India a vast and thickly populated country but also the people who live here are ethnically heterogeneous. This heterogeneity is manifested in significantly different religions, communities, castes, cultures, languages (18 major languages and more than 200 dialects!), food habits, lifestyles and genetic endowment. It can be said that India has diversity comparable to the whole of Europe and this diversity must be taken into account while planning any program. It is hardly possible for any researcher to know all local languages. To plan a research program involving a number of interpreters is not only cost prohibitive but also time consuming and will make planning the schedules more difficult. Hence the usual way is to find a compromise by which the exchange of ideas can take place without much hindrance. A large number of Indians are illiterate and they are reluctant to put their thumb impression or signature out of apprehension. A local leader acts as their guardian and he has his own choices and wishes, which manifest in the long run. Thus any activity that requires the use of free will by and willing consent of, the volunteers is vetted by their leaders. While working in some villages in West Midnapore district, where few Telegu-speaking people live, to overcome the language barrier a local Telegu-speaking person was appointed as an interpreter, on the instruction of the local panchayat leader (elected representative of the gram panchayat ). The panchayati raj is a three-tier system of rural local self-government in India and it links a village to the district. The panchayati raj institutions are accepted as agencies of public welfare. All developmental programs are channeled through these bodies. The members of these institutions are elected by people's verdict. Panchayati raj institutions strengthen democracy at its root and ensure more effective and better participation of the people in the government. The three tiers in the panchayati raj institutions are - a) gram panchayats, which operate at the village level; (b) panchayat samities, which operate at the block level (each block is a collection of several villages); and (c) zilla parishads, which operate at the district level. In this way, development of districts (assemblies of various blocks) is carried out democratically. To the utter surprise of researchers, money was demanded at the end of the research program, asserting that they were promised by the interpreter of payment at the end of the program (violation of principle of non-exploitation and principle of accountability and transparency. ICMR, in its general guidelines item 3, points out the principle of non-exploitation, whereby, as a general rule, the subjects are remunerated for their involvement in the research. Each research shall include an inbuilt mechanism for compensation of human subjects, either through insurance or other appropriate measures. ICMR, in its general guidelines item 7, also points out the principle of accountability and transparency, whereby the research or experiment will be conducted in a fair, honest, impartial and transparent manner after those associated with the research make full disclosures with respect to the research or experiment). Economic gaps Economic realities were taken into consideration. This included both the finances to make comprehensive and acceptable disease-care services available to the people; and, more importantly, the capacity of the people to afford these services. The Indian government spends around 1.2% of its annual budget on health and as communicable disease prevention and management is still an important aspect of health care in India, the money routinely allocated to noncommunicable diseases, especially diabetes, is sparse.[2] As already discussed, rural Bengal lacked the proper infrastructure of health care management. A vicious cycle of 'poverty, malnutrition, ignorance, lack of moral values, perpetual poverty' was at the root of such a state of affairs. Due to poverty, rural people were not only susceptible to diseases but also could not avail of the prevailing health infrastructure. The 1998 Nobel Prize winner for Economics, Amartya Sen, said in the context of famines, 'the root cause of starvation in famines is not the lack of food, but the capacity of the average person to buy food.'[3],[4] It could be said that the root cause of failure of a 'diabetes program' was not only the non-availability of services, but also the inability of the average person to afford these services, wherever available. The per capita income of an Indian was estimated in 2005 to be Rs. 15,000 per year. In view of the significant disparity in incomes, most people actually earned much less, the situation being even worse for the rural population. According to the 1998 World Development Report, 52% of the Indian population lived below the accepted poverty line. This was based on the rupee value vis-à-vis the dollar at the 1985 rate of around Rs. 14 to the dollar, whilst it was around Rs. 43 to the dollar in 2004. Consequently, the number of people living below the poverty line was estimated by economists to be more than 75%.[3] The Inequality Index in India is extremely high and this again showed that the real per capita income was much less than that reported amount of Rs. 15,000 per year.[2] Presence of big economic gaps in the society and loss of moral values in villages due to socio-political factors led to growing dissatisfaction and disharmony and to alienation, where anybody living in a better economic condition in a town was viewed as a symbol of affluence and a person of vested interest from whom money should be extracted by all means. Out of the 62 gram panchayats where the work was done, 8 panchayats asked for money for giving written consents and 26 panchayats flatly refused. The situation smoothened and eased up if a researcher held a common political belief. In many gram panchayats, the members of the team of researchers were asked about their affiliation to political parties and different members of the team had to pose as supporters of different political parties according to the scenario of the villages. This violated in stricter sense the principles of accountability and transparency. Further, village politics of West Bengal was segregated in groups and researchers were pressurized by some panchayats to release confidential information of persons belonging to other groups in exchange of greater cooperation (violation of the principle of confidentiality and privacy, of ICMR. In item 4 of general guidelines, ICMR states the principle of confidentiality and privacy, whereby identity and records of human subjects for the research or experiment are kept confidential and are not disclosed without consent in writing). Volunteers X, Y, Z, M, N gave written consents in a diabetic research program in which the effects of 100 g/day of fenugreek were observed. They stayed in a village in one area of Midnapore East district. Fenugreek is commonly used as a condiment in rural Bengal and is commonly known as methi. The local panchayat did not allow the said work to be done as the authors refused to pay bribes to the panchayat members. Further, the research team was asked to predict that no disease would occur in the volunteers at any time in the future, even after the period of study and refusal to yield resulted in threats with unforeseen consequences. Cultural gaps India has a wide variety of cultures, characteristic to different religions, races and tribes. Sometimes the food of one group was prohibitory to another and hence research planning could not be uniform. Any research involving family planning activities are prohibitory to Islam. A uniform gradient of a research process was tough and not achievable. Communal approaches and inter- and intra-religious conflicts further eluded uniformity. Moreover, the rural-urban divide among the people also seems to be an important factor. Around 70% of the people live in rural areas and 30% in urban surroundings. Rural to urban shift of population is an ongoing phenomenon. Even in the so-called urban milieu, considerable differences exist between those living in major cities and those living in smaller towns. It is rarely appreciated that there is a significant diversity amongst people living in rural, semi-urban and urban areas. Whilst the ultimate goals of a disease-care program may be the same, the differences and diversities must be taken into account when drawing up specific plans and guidelines to be put into effect in order to achieve the objectives. 3) Principle of essentiality entails the use of human subjects for research and villagers in one gram panchayat were asked to eat specially prepared rice containing a higher percentage of retrograded starch to observe its blood sugar lowering activity. To the utter surprise of researchers, the villagers protested saying that the research was not essentially meant for them as diabetes was thought to be a disease which affected only the rich and affluent. Some panchayats (four in number) even argued that the principle of the maximization of public interest and of distributive justice ( vide ICMR general guidelines item 8, which states the principle of the maximization of public interest and of distributive justice, whereby the benefits of research will be distributed equally among mankind) was violated by any research process in India as the benefits of the research would not be distributed equally to mankind in India and they were opposing activities in which poor villagers would be the volunteers while the beneficiaries would be rich urban people. They argued that even the monetary compensation provided was inadequate. 4) The principle of non-exploitation as directed by ICMR dictated that each research should include an inbuilt mechanism for compensation of human subjects, either through insurance or other appropriate measures (ICMR, in general guidelines item 3, defines the principle of non-exploitation, whereby, as a general rule, the subjects are remunerated for their involvement in the research. Each research shall include an inbuilt mechanism for compensation of human subjects either through insurance or other appropriate measures). These panchayats went beyond ICMR guidelines and demanded royalty, like royalty on monetary transactions from outcomes of research. The implementation of the principle of precaution and risk minimization, whereby due care and caution is to be taken at all stages of the research and experiment to ensure minimum risk to volunteers, as guided by ICMR was ensured; but these panchayats were unyielding in spite of being provided with documented proofs of complying to all necessary guidelines of research and persisted on their demand for monetary compensation as royalty, causing abandoning of the program in those villages (ICMR, in general guidelines item 5, defines the principle of precaution and risk minimization, whereby due care and caution is to be taken at all stages of research and experiment to ensure minimum risk to volunteers). 5) Three panchayats asked for ICMR or other guidelines and demanded in writing that all the guidelines would be complied with; and when this was done, they inquired about the principle of professional competence and the principle of accountability and transparency (ICMR, in general guidelines item 6, states the principle of professional competence, whereby only professionals who are having requisite qualifications and competence conduct research at all stages). The authors conducted studies to evaluate the effects of various nutraceuticals in volunteers and one such study involved flaxseed oil, directed to be used as salad oil. As this was not a commonly consumed oil, some volunteers tricked the researchers by using this oil to feed cattle, after learning that the oil was beneficial for cattle. Two panchayats in one block in Midnapore West district had posed several problems to researchers. The panchayats there were mainly controlled by adivasis, who had their own beliefs, cultures, values, customs and taboos.[5] Over the years, the tribal community developed an intimate knowledge of various plants and their medicinal uses and they had strong faith in these.[6] These panchayats handled the issue in an arrogant way and said that the entire work should be supervised by the local health care provider, who was not a qualified doctor. The areas under these panchayats were economically backward areas and all the tricks were initiated by the local quack, who was apprehensive of losing his income. The problem of untouchables and castes prevailed in some people in two panchayats and team members were asked about their caste by a few volunteers before they agreed to give written consents. Socio-political difficulties ICMR criteria for monetary compensations are very strict and limited to reimbursement only for inconvenience and time spent in connection with participation in research; such payments should not cause inducement of their decision to participate in the research against their better judgment. Institutional Ethics Committee (IEC) approves all payments and reimbursements, including that for medical services. IEC looks after conflicts of interests between scientific responsibilities of researchers and business interests in case of sponsored projects. According to ICMR guidelines, (a) a guardian giving consent on behalf of an incompetent person is entitled for only pocket expenses, (b) a subject withdrawing for medical reasons from the research should get the benefit of full participation, (c) the person withdrawing for any other reasons should be paid in proportion to the extent of participation, (d) undue inducement through compensation for individual participants, families and populations is prohibited. This prohibition does not apply to agreements with families, individuals, groups, communities and populations that foresee technology transfer, local training, joint ventures, health care reimbursements, costs of travel, loss of wages and percentage of royalties for humanitarian purposes. If the quality of human capital is not good, physical capital and natural resources cannot be properly utilized and growth will neither be sustainable nor qualitative. Health is a major segment of human capital. According to WHO, health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.[7] Health status is usually measured in terms of life expectancy at birth, infant mortality rate, fertility rate, crude birth rate and crude death rate. These indicators of health are determined by numerous factors such as per capita income, nutrition, housing, sanitation, safe drinking water, social infrastructure, health and medical care services provided by government, geographical climate, employment status, incidence of poverty and the like.[8],[9] It is, de facto, the quality of human health upon which the realization of the goals of life and objectives of a person, community or nation as a whole depends. Health is a multidimensional phenomenon. It is both an end and means of development strategy. The relationship between health and development is mutually reinforcing - while health contributes to economic development, the latter, in turn, tends to improve the health status of the population in a country. Health is also an important entitlement that enhances 'capabilities' of the poor people, leading to increase in 'commodities' and further improvement in health status.[9],[10] As investment on health increases, the productive capacity of the working population and hence the level of income, tends to rise and to that extent it contributes to a decline in the incidence of poverty.[8] With rapid improvement in health, particularly of the poor, the 'vicious cycle' of poverty can be converted into a 'virtuous cycle' of prosperity.[10],[11],[12] Although there has been a two-way relationship, a strong causal link from adult health to economic growth is observed by many studies.[11],[13],[14] Knowles and Owen in the year 1997 and Jamison and Wang in the year 1998 contend that life expectancy contributes to economic growth more than education. In addition to its direct impact on productivity, health has other effects on economic development and demographic transition.[13],[14] The stringent criteria of ICMR regarding monetary benefits given to the subjects of research or experiment are owing to poverty in rural India so that the experimenter does not induce impairment of judgments and provocation in the volunteers by paying money. However, while doing clinical trials in rural Bengal, an experimenter confronts different experiences. Enhanced political involvements of the village population in Bengal lead to political polarizations, whereby sections of village people are privileged in terms of social and economic development. Further, the panchayats are the supreme decision-making authority at the village level. So for any research involving volunteers in rural Bengal, panchayats play a prominent role in regulating the conditions and many times put large constraints to maintaining the ethical guidelines of ICMR. Political approaches may be required to influence the panchayats and research of any kind requires to be approved by panchayats , though they may not hold any official sanction. At the individual level, money shapes a big deal. Villagers put complex demands even when the research involves minimum risk. They usually demand money for each step, even after the steps of research are clearly explained as per existing ICMR rules. Frequently, the villagers, being influenced by others, like family members, local leaders ( panchayat pradhans ), change their mind and as local leaders are all-powerful, they usually never confront them, even disregarding their earlier commitments. Their ignorance may hinder acceptance. While conducting researches on nutraceuticals, even observing the effects of rice, which is the staple food in Bengal, was objected to by panchayats and money was demanded.[15] More or less, the social structure has so changed that a researcher is viewed as an outsider and an affluent man of city and many unwanted demands, including those of money, jobs, clothes, household belongings, etc, ethically not permitted by ICMR, are put to him. A researcher is left to act depending on his wisdom and judgment. ICMR should be more practical in framing the ethical guidelines, as the scenario is more or less the same throughout India, particularly in eastern India.[16],[17] Barden and Boyer, in the year 1993, suggested that the research methods be extended to include intuitive, spiritual and personal categories of understanding. They suggested four areas of focus to evaluate the new scholarship: importance of the research, integrity of the process, explanation of the methodology and acknowledgment of research limits.[18] Inadequacy of heath structure Mounting patient load is taking its toll on research activities at the Postgraduate Institute of Medical Education and Research. Growing clinical load at the PGI's OPDs apart (on an average about 4,000 old and new patients visit daily), the waiting period for any surgery at the institute ranges from 2 weeks to 3 months, depending upon the availability of finances and redress of other critical factors.[19] In all hospitals, doctors are overloaded and time for research is wanting. As a result, the doctors cannot even communicate their research work for publication in time. This resulted in the doctors' noncompliance with ICMR guidelines regarding principles of public domain and with regard to reporting to Institute Ethical Committee within the stipulated time. (ICMR, in its general guidelines item 10, states the principle of public domain, whereby the research and any further researches are generally to be made known through scientific and other publications, considering the law of the land at the time). Further, this indirectly compelled noncompliance with the principle of totality of responsibility, whereby the professional and moral responsibility in respect of the research devolves on all those directly or indirectly connected with the research (item 11 of general guidelines of ICMR). Further, business houses frequently compel the researcher/clinician to yield to their demands as patent laws and other laws pertaining to 'R and D' activities in the land are in the budding stage. In many institutions, IEC makes unusual delay to give permission for research and the researcher is compelled to be a silent spectator to the delay, even for a research program that involves minimum risk. The present team of researchers faced the same difficulties and one leading multinational company proposed to buy the technological outcomes, pointing to the complex nature of law of the land. Yielding to such pressure would violate the principle of compliance (ICMR, in its general guidelines item 12, states the principle of compliance, whereby the guidelines for research as per existing rules and norms laid down by competent authorities as per existing laws of the land are to be complied with by all involved in research). Stringency of audit India suffered in colonial rule. The basis of colonial rule was not to trust the Indians at large and hence make all financial transactions complicated and clumsy. To procure items of research or to make any payment on demand of situation, prior approval of the concerned authority was a 'must,' and by the time approval came, the interest in work was lost. The situation has hardly changed in free India, even after over half a century since independence. Conclusion Money and monetary gains are nowadays considered as the principal motivating factors. Other important ambition is that of acquiring power. More frequently than not, politics is in nexus with money and power and is oriented towards personal gain. A Panchayat Pradhan , though being a part of the society, in most cases looks after his own short-term gains. He perhaps possesses neither the wisdom nor the knowledge to enable him to appreciate the impact of good research. Any act of research in his domain allows him to exercise his power and he does exercise it to satisfy his ego and/or for his convenience. A research activity should be looked after by such persons who have sufficient knowledge and know what research is and how research helps mankind. As a further conclusion, the authors suggest ICMR should have a fresh look at the guidelines and incorporate changes where necessary, taking into consideration the ground realities. References
Copyright 2006 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms06072a1.jpg] |
| |||||||||

{kind=link}