 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
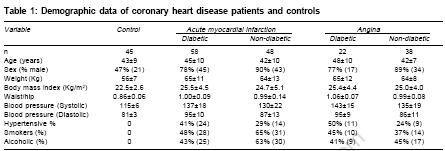
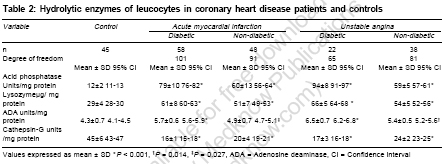
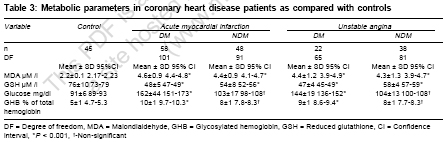
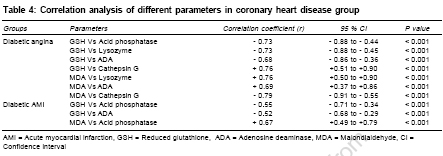
Indian Journal of Medical Sciences, Vol. 61, No. 2, February, 2007, pp. 73-82 Original Contributions Study of leukocytic hydrolytic enzymes in patients with acute stage of coronary heart disease Chavan Vishwas, Patil Neela, Karnik ND Department of Biochemistry, LTM Medical College and General Hospital, Mumbai - 400 022 Code Number: ms07013 Abstract BACKGROUND: Coronary heart disease (CHD) is a major killer worldwide. Atherosclerosis, which is the basis of CHD, is believed to be an inflammatory disorder. Though various aspects of atherosclerosis are extensively studied, leukocytic hydrolytic enzymes are not studied very well with respect t°CHD.AIM:This study was planned to assess changes associated with leukocytic hydrolases in CHD patients. SETTING AND DESIGN: A tertiary care hospital; case-control study. MATERIALS AND METHODS: 106 patients with acute myocardial infarction, 60 patients with unstable angina and 45 healthy controls were included in the study. Acid phosphatase, lysozyme, adenosine deaminase (ADA) and cathepsin-G levels were estimated from leukocytes. Reduced glutathione (GSH) and malondialdehyde (MDA) levels were measured. STATISTICAL ANALYSIS: Statistical comparison of data was done using student's t-test (unpaired). Correlation difference was calculated by using Pearson correlation coefficient. RESULTS: Significantly higher levels of acid phosphatase, lysozyme, ADA with lower levels of cathepsin G in leukocytes were observed in CHD group. We also found significantly higher levels of serum MDA with lower concentrations of blood GSH in CHD group. In diabetic CHD group, significantly higher levels of leukocytic acid phosphatase, lysozyme, ADA and serum MDA with lower levels of cathepsin G and blood GSH were observed. CONCLUSIONS: Our study indicates that leukocyte hydrolytic enzymes, mainly acid phosphatase, lysozyme and ADA were more active in CHD patients and may contribute to inflammation related with CHD. Its also indicates that leukocyte cathepsin-G may have antiinflammatory role. Keywords: Coronary heart disease, hydrolytic enzymes, inflammation, leukocytes Introduction Atherosclerosis, which is the basis of coronary heart disease (CHD), is believed to be an inflammatory disorder. Inflammation must smolder for decades before resulting in a clinical event like angina or acute myocardial infarction (AMI).[1] Generation of free radicals and oxidative stress may have an important role in atherogenesis.[2] In inflammation, leucocytes rapidly produce free radicals. If free radicals remain in the body for longer time, they can damage body cells. AMI is frequently associated with leukocytosis and an elevated peripheral neutrophil count. It was shown that stimulated leucocytes can modify LDL, which can contribute to atherogenesis.[3] Also, many risk factors of CHD like diabetes mellitus have relation with inflammation. One link between inflammation and the incidence of type 2 diabetes may be insulin resistance. Several mechanisms may explain the relation between insulin resistance and inflammatory factors, such as the hypersecretion of proinflammatory cytokines like interleukin-6 and tissue necrosis factor-Ü, from adipose tissue. These cytokines exert stimulatory effects on the synthesis of acute phase proteins.[4] Though inflammation has such an importance in atherosclerosis, leucocytes which are integral part of inflammatory process, are not studied intensively. Hence, we studied leukocytic hydrolytic enzymes in CHD, which may have significant role in the inflammatory aspect of atherosclerosis and consequently in cardiovascular diseases. Materials and Methods Materials Micrococcus lysodeikticus and lysozyme standard were purchased from Sigma Chemicals Co, USA. N-Succinyl-L-Alanyl-L-Alanyl-L-Prolyl-L-Phenylalanine-4-nitroanilide (substrate for cathepsin G) was obtained from Fluka laboratories, USA. P-nitrophenyl phosphate and reduced glutathione were obtained from Sisc°Co. All other chemicals and solvents used were of analytical reagent grade and obtained locally. Patients 166 patients, [139(84%) men and 27(16%) women] with the diagnosis of AMI or unstable angina, registered in our hospital between January 2002 and December 2004 were selected for study. The diagnosis of AMI was established according to clinical criteria: chest pain, which lasted for up to 3 hours, ECG changes (ST elevation of 2 mm or more in at least two leads) and CPK elevation. The diagnosis of unstable angina was established according to clinical criteria: chest pain and ECG changes. The diagnosis of hypertension was based on previous history of hypertension or systolic blood pressure > 140 mm of Hg and diastolic blood pressure > 90 mm of Hg on minimum two measurements. The diagnosis of diabetes was based on previous history of diabetes mellitus or fasting blood sugar more than 126 mg/dl or random blood sugar more than 200 mg/dl. All the diabetic CHD patients included in the study (80) were on oral hypoglycemic agents. A person was considered smoker or alcoholic based on his history of smoking or alcohol consumption. The control group consisted of 45 healthy, age-matched subjects, 21 men and 24 women, recruited from an annual check-up program. Age of patients and control subjects were between 25-50 years. Inclusion criteria Patients below 50 years of age, with diagnosis of angina or AMI and free from any kidney or liver diseases. Exclusion criteria Patients above 50 years of age, with any kidney or liver diseases and pregnancy. Ethics committee of our hospital gave approval and informed consent was obtained from every patient. Isolation of leukocytes Samples were collected after overnight fasting in EDTA bulbs and leucocytes were isolated by established procedure.[5] 5.0 ml of anticoagulated blood was mixed with 1.0 ml of freshly prepared 5% dextran solution and allowed to stand for 45 minutes. Supernatant was removed and centrifuged at 500 rpm for 10 min. in cold condition. Leukocyte pellet obtained was mixed with 1.5 ml ice-cold distilled water and then 1.5 ml ice-cold 1.8% NaCl solution and centrifuged at 500 rpm for 10 min. in cold condition. Isolated leukocyte pellet was suspended in one ml of ice-cold normal saline. Leukocytic enzymes determination Leukocyte pellet with ice-cold saline was transferred to a smooth walled homogenizing vessel and disrupted with a loose fitting motor driven Teflon pestle with 10 strokes. The homogenate was centrifuged at 3000 RPM for 10 min and supernatant was used for the hydrolytic enzymes estimation. Acid phosphatase activity was determined by its action on p-nitrophenyl phosphate, which results in release of p-nitrophenol which is then quantified at 405 nm.[6] Results were expressed as units/mg of protein. The assay of lysozyme was based on the lysis of Micrococcus lysodeikticus cells by lysozyme, which causes decrease in absorbance of substrate at 450 nm.[7] In a substrate containing Micrococcus lysodeikticus , sample or standard was added and readings were taken at 30 seconds and 10 minutes. Difference between two readings is calculated. Results were expressed as mg/mg of protein. Adenosine deaminase (ADA) activity was estimated by its action on substrate containing adenosine. Principle of reaction is Berthlot reaction. Readings were taken at 640 nm. 1 unit of activity corresponds to the amount which liberates 1 mg of ammonia nitrogen/ml of sample/hour at 37°C.[8] Results were expressed as units/mg of protein. Cathepsin-G activity was determined by hydrolysis of substrate (N-Succinyl-L-Alanyl-L-Alanyl-L-Prolyl-L-Phenylalanine-4-nitroanilide) by cathepsin-G.[9] In a cuvette, substrate and sample was mixed at 50°C. Amount of p-Nitrophenol liberated was measured at 410 nm. Results were expressed as units/mg of protein. Protein estimation was carried out according to Lowry et al with crystalline bovine serum albumin as standard. Sample was allowed to react with Folin-Ciocalteu reagent, taking reading at 660 nm.[10] Results were expressed as mg/ml. MDA[11] levels were determined by their reaction with 2-Thiobarbituric acid (TBA). Protein were precipitated by adding 40% trichloroacetic acid and then 0.67% TBA was added. Mixture was boiled for 60 minutes. Pink colour developed was extracted in n-butanol and read at 533 nm. 1, 1, 3,3- Tetramethoxy propane was used as a standard. Results were expressed as µM/l. GSH levels were estimated by reaction with 5, 5′- dithio-bis-(2-nitrobenzoic acid) [DTNB].[12] Proteins were precipitated from blood by adding a reagent containing sodium chloride, EDTA and meta-phosphoric acid. Mixture was filtered and filtrate was allowed to react with DTNB. Yellow colour developed was read at 412 nm. A standard was included in the test. Results were expressed as µM/l. GHB[13] levels were determined by their reaction with TBA. Red blood cells were thoroughly washed with saline and then hydrolyzed with oxalic acid (i.e., hydrolysis of hexoses bound to hemoglobin) whereby 5 hydroxymethyl furfural is liberated. After precipitating proteins, the supernatant was allowed to react with TBA at 37°C for 40 min. The yellow colored TBA - 5 - hydroxymethyl furfural adduct formed was measured at 443 nm in a spectrophotometer. Results were expressed as % of total hemoglobin. Glucose levels were determined by GOD-POD method using kit supplied by Accurex, India. Statistical analysis The data from patients and controls were compared using unpaired student′s t-test and values were expressed as means ± standard deviation (SD). Correlation analysis was done by using Pearson correlation method. Sigma stat version 3.0 was used for statistical analysis. Results General characteristics of CHD patients and controls are shown in [Table - 1]. The table shows that age of CHD patients was less than 50 years. Percentage of male CHD patients was more than female CHD patients. The table shows higher BMI and waist to hip ratio in patients as compared to controls, marking importance of obesity in CHD patients, though elevation is not significant. Systolic and diastolic blood pressures (B.P.) were increased in CHD patients than in controls. Number of hypertensive patients were more in diabetic group. [Table - 2] shows activities of 4 different hydrolases of leukocytes in CHD patients as compared to control subjects. Acid phosphatase and lysozyme values were significantly higher in CHD patients, as compared with controls ( P < 0.001). ADA values were significantly high in diabetic CHD patients ( P < 0.001). Cathepsin-G values were significantly low in CHD patients ( P < 0.001). [Table - 3] shows metabolic parameters in CHD patients and controls. MDA levels were significantly higher while GSH levels were significantly lower in diabetic as well as non-diabetic patient group ( P < 0.001). Glucose and GHB levels were significantly higher in diabetic CHD group ( P < 0.001). [Table - 4] shows correlation analysis between different parameters in the patients groups. Leukocyte acid phosphatase, lysozyme and ADA levels were found to be positively correlated and cathepsin G activity was negatively correlated with MDA, a lipid peroxidation product. Also, Leukocyte acid phosphatase, lysozyme and ADA activities were negatively correlated and cathepsin G activity was positively correlated with GSH, a well known antioxidant. Discussion The root cause of CHD is mainly atherosclerosis. Inflammation, oxidative stress, antioxidants and leukocytic hydrolases has important role in pathology of atherosclerosis. Yoshikawa et al found that the increase in lipid peroxide causes the instability of lysosomal membranes and releases various kinds of hydrolytic enzymes, which can lead to further cell damage.[14] In our study, we found significant increase in leukocyte hydrolytic enzymes, namely acid phosphatase, ADA and lysozyme, in patient group, suggesting their role in inflammation involved in CHD. We also found significant decrease in leukocyte cathepsin-G activity, indicating antiinflammatory role of this enzyme. Acid phosphatase Acid phosphatase (EC 3.1.3.2) is a marker enzyme, used for the study of lysosomal enzyme activity.[15] Acid phosphatase activity is found in monocytes, lymphocytes and neutrophils. In our study, we found significantly higher activity of acid phosphatase in leukocytes of CHD patients than that of control subjects, which suggests that at least some hydrolytic enzymes are abnormally active in CHD and atherosclerosis. Hoen et al found that in chronic vitamin C deficiency, lysosomal acid phosphatase activity was increased.[16] Leveille et al found that the activity of lysosomal acid phosphatase was significantly elevated in animals on low vitamin C diet, which indicated an inverse relationship between vitamin C concentrations and lysosomal enzyme activities.[17] In our study, leukocyte acid phosphatase was positively correlated with MDA and negatively correlated with GSH, confirming results of above studies. Lysozyme Lysozyme (EC 3.2.1.17) catalyzes the hydrolysis of polysaccharide chains that form structural elements of bacterial cell walls. Significant rise in lysozyme activity ( P < 0.001) in patient group as compared to controls, suggests that lysozyme may be involved in inflammatory process in conjunction with unstable angina and AMI. Increased lysozyme activity may be considered as a part of systemic inflammatory response, as suggested by previous work of Hickey et al .[18] This was supported by our findings that lysozyme was positively correlated with MDA and negatively correlated with GSH. Adenosine deaminase (ADA) ADA (EC 3.5.4.4) catalyzes the conversion of adenosine to inosine and 2′-deoxyadenosine to 2′-deoxyinosine. The major source of serum ADA may be lymphocytes or the monocyte-macrophage cell system. It was reported that elevated levels of ADA reflect the changes in the immune response in the pathogenesis of atherosclerosis and CHD. Hence ADA can be considered as important marker in assessing CHD.[19] Also, ADA is considered as an inflammatory marker in rheumatoid arthritis[20] and in the mouse model of pleurisy.[21] In our study, we found significantly elevated leukocyte ADA levels in CHD patients, which is similar to work of Kopff et al , who found that plasma ADA activity is increased in patients with unstable angina.[22] Positive correlation found between leukocyte ADA and MDA as well as negative correlation with GSH suggest that ADA may serve as an indicator of underlying inflammation. Cathepsin-G Our results showed significantly lower values of leukocyte cathepsin-G (EC 3.4.21.20) in CHD patients, than control subjects. Cathepsin-G is a component of the azurophilic granules of human neutrophils. In inflammation, leukocytes release hydrolytic enzymes. Cathepsin-G, which is also a hydrolase, may have a role in inflammation. In 1985, Reilly et al suggested that cathepsin-G can inactivate bradykinin and thus may play an important role in the down-regulation of acute inflammation.[23] Studies by Bank et al in 1999 and 2000 showed that cathepsin-G inactivates interleukin-6 at the site of inflammation.[24],[25] Both bradykinin and interleukin-6 are well-known inflammatory mediators. Thus it may be possible that cathepsin-G can act as an anti-inflammatory molecule. Another possibility is that cathepsin-G may be consumed during the complex interactions between different enzymes, during the inflammatory process. Shao B et al demonstrated that oxidants from leukocytes inactivate cathepsin-G.[26] Our results showed significantly lower values of cathepsin G in patient group ( P < 0.001) and decrease was more pronounced in diabetic CHD group. This indicates that cathepsin G level is susceptible to glucose control. In our study, cathepsin-G was negatively correlated with MDA and positively correlated with GSH. This indicates that cathepsin G is susceptible to oxidative stress status. GSH is a well known antioxidant, negative correlation with acid phosphatase, lysozyme and adenosine deaminase indicate possible inflammatory role of these hydrolases in CHD, at least in diabetic CHD. Similarly, MDA is a well known lipid peroxidation product. Hence, positive correlation suggested possible role of these hydrolases in oxidative stress, at least in diabetic CHD condition. This also indicates that these hydrolases are more active in diabetic CHD patients. Also, positive correlation of cathepsin G with GSH and negative correlation with MDA, suggests possible anti-inflammatory role of cathepsin G. Effect of various factors No significant difference was found between results of male patients and female patients, suggesting that gender don′t have significant effect on leukocyte hydrolase activity. Hypertension, smoking, BMI are important confounding factors, but results were more or less similar after adjusting for these important parameters. Increase in acid phosphatase activity is mostly considered with prostate cancer, but none of our CHD patients had any abnormality of prostate gland, as indicated by through medical history. Medications given to patients may affect the results. Many patients are thrombolysed and treated with heparin and aspirin. It was shown that heparin have anti-inflammatory effect and may affect leukocyte function.[27] Similarly, it is known that after AMI, aspirin is associated with lower levels of inflammatory markers.[28] Strengths and limitations of study and future research directions This study suggests a relatively new approach t°CHD. Hydrolytic enzymes of leukocytes, which are poorly studied in CHD patients, provide new insights in the role of leukocytes in CHD. These enzymes can be used as measures of inflammation associated with CHD and can be beneficial to patient′s care, when controlled. Adanin et al suggested that inhibition of ADA might be a novel and viable therapeutic approach to manage the systemic inflammatory response.[29] But, as number of samples is less in our study, extensive studies with larger number of samples are needed to confirm exact role of these enzymes. Also, study of different cell lines of leukocytes (neutrophils, monocytes etc) and their enzymes may provide a detailed view of still unexplored area of CHD and atherosclerosis. Conclusion Our study indicates possible inflammatory role of leukocyte hydrolytic enzymes, mainly acid phosphatase, lysozyme and adenosine deaminase and antiinflammatory role of cathepsin-G. In conclusion, it is possible that inflammation, oxidative stress and diabetes have profound effect on internal environment of leukocytes, which causes disturbed balance between hydrolytic enzymes, which may have significant role in atherosclerosis and CHD. References
Copyright 2007 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms07013t4.jpg] [ms07013t3.jpg] [ms07013t1.jpg] [ms07013t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}