 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
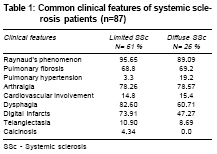
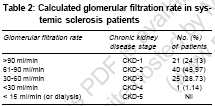
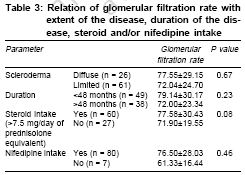
Indian Journal of Medical Sciences, Vol. 61, No. 2, February, 2007, pp. 91-96 Original Contributions Prevalence of renal involvement in Indian patients with systemic sclerosis Gupta R, Bammigatti C, Dinda AK, Marwaha V, Gupta S Department of Medicine, All India Institute of Medical sciences, New Delhi Code Number: ms07015 Abstract Background: Renal involvement in systemic sclerosis (SSc) either in the form of scleroderma renal crisis (SRC) or nonrenal crisis abnormalities has been reported to be in the range of 60-80%. Renal involvement is thought to be rare in Indian patients with SSc. However, there is paucity of data.Aims: To study the frequency and pattern of renal involvement in Indian patients with SSc. Settings and Design: A single center prospective, cross sectional study. Materials and Methods: We prospectively evaluated the patients with SSc attending the Rheumatology Clinic. All patients were evaluated for renal involvement. All patients underwent measurement of blood pressure, urine examination, glomerular filtration rate (GFR) estimation using Cockcroft-Gault formula and kidney biopsy when indicated. Statistical Analysis: Statistical analysis was performed using SAS 8.0 statistical package. Results: Eighty-seven patients were included in the study from July 2001 to December 2004. Mean age of patients was 36.88 ± 12.51 years. About 30% of patients had diffuse cutaneous SSc. None of these patients had SRC either at enrollment in the study or during follow-up. Eleven (12.6%) patients had hypertension. Six (6.9%) patients had abnormal urinary findings in the form of either active urinary sediment or significant proteinuria. Only one patient had azotemia (plasma creatinine > 1.8 mg/dl). Calculated GFR < 90 ml/min was seen in about 75% patients, out of these about 30% patients had chronic kidney disease. Conclusion: SRC is very rare in Indian patients with SSc. However, non-renal crisis abnormalities appear to be as common in Indian patients as compared to the western literature. Keywords: Renal involvement, scleroderma renal crisis, systemic sclerosis Introduction Renal involvement in scleroderma can be divided into scleroderma renal crisis (SRC) and non renal crisis. Moore and Sheehan in 1952 first described SRC which is characterized by renal insufficiency (serum creatinine ≥ 2.0 mg/dl or a doubling of serum creatinine above the value at baseline, in the absence of another defined cause) and/or malignant hypertension (systolic blood pressure ≥ 160 mm Hg or diastolic blood pressure ≥ 110 mm Hg on at least 2 occasions, a minimum of 12 hours apart), accompanied by persistent urinary abnormalities or evidence of microangiopathic hemolytic anemia.[1] SRC occurs in approximately 10% of all scleroderma patients. Patients with diffuse scleroderma are at greatest risk, with upto 20% to 25% of these patients developing SRC.[2] SRC is most often encountered early in the course of the disease, with 75% of SRC cases occurring less than 4 years after the first symptom attributable to scleroderma. SRC occurs more commonly in black patients and males are affected more frequently than females.[3] SRC was the most deadly complication of SSc and renal failure was the leading cause of death in systemic sclerosis (SSc) until the advent of effective therapy. Over the last few years, the outcome of SRC has improved dramatically with the use of angiotensin-converting enzyme inhibitors.[3] Nonrenal crisis abnormalities are also seen in large number of patients with SSc. Frequency of nonrenal crisis abnormalities, in the form of hypertension, azotemia or proteinuria is said to be as high as 45% to 60%.[4] Renal involvement is said to be uncommon in Indian patients with SSc.[5] We too feel that renal involvement is rare in Indian patients with SSc. Since, there is paucity of data from Indian subcontinent; we conducted this study to evaluate the frequency of renal involvement in Indian patients with SSc. Materials and Methods Patients The study population included 87 consecutive patients with SSc attending rheumatology clinic, from July 2001 to December 2004. All patients fulfilled the American College of Rheumatology (ACR) criteria for SSc.[6] The disease was classified as diffuse SSc if sclerodermatous changes were present in the proximal extremities and trunk or limited SSc if proximal extremities and trunk were not involved.[7] The disease onset was defined as the onset of first symptom attributable to SSc. This was a single center, prospective cross-sectional study conducted to evaluate the frequency of renal involvement in Indian SSc patients. All patients gave written informed consent for the enrollment into the study. Department protocol committee approved study protocol. All patients were evaluated as per the pre-designed protocol. Detailed history and physical examination were followed by relevant investigations to note the extent of the organ involvement. Assessment of renal involvement All patients were carefully evaluated to look for the renal involvement, with history suggestive of SRC in the past, measurement of blood pressure recordings, urine examination for the presence of proteinuria or active sediment, measurement of serum urea and creatinine concentration and calculation of Creatinine Clearance using Cockcroft-Gault formula i.e. Creatinine clearance (ml / min) = (140 - age) x lean body weight (KG) Plasma creatinine (mg/dl) x 72 A factor of 0.85 was used for females.[8] Kidney biopsy was done in patients with the active urinary sediment and/or persistent nephrotic range proteinuria (≥ 3.5 grams/day). Patients were considered hypertensive if they had blood pressure recording> 140/90 mmHg on the basis of the average of> 2 readings taken at each of two or more visits after an initial screening.[9] Based on the calculated glomerular filtration rate (GFR), chronic kidney disease was classified as stage 2 when GFR is between 60-89 ml/min, stage 3 when GFR is between 30-59 ml/min, stage 4 when GFR is between 15-29 ml / min and kidney failure when GFR is < 15 ml/min or requiring regular dialysis.[10] Statistical analysis Statistical analyses were performed using SAS 8.0 statistical package. All continuous variables were expressed as mean ± SD, whereas categorical variables were expressed as frequencies and their percentages. Student t test was performed to see the association between continuous variables, whereas Chi-square test was performed to see the association between categorical variables. P value of ≤ 0.05 is considered as significant. Results A total of 87 patients were included in the study. Mean age of our patients was 36.88 ± 12.51 years and majority of our patients were females with female: male ratio being 7.7: 1.0. Mean duration of symptoms at the time of presentation in our patients was 62.70 ± 53.13 months. Twenty-six (29.88%) patients were classified as having diffuse Scleroderma and 61 (70.11%) patients were classified as having limited Scleroderma. Raynaud′s phenomenon was the most common symptom, which was seen in 76 (88.4%) patients. Other common clinical features are shown in [Table - 1]. Antinuclear antibody positivity was seen in 73 (83.9%) patients. Renal involvement None of the 87 patients had SRC either at enrollment into the study or during follow up period. Eleven (12.6%) patients met the criteria to be classified as having arterial hypertension. Of the 11 patients who had hypertension, only 5 (5.7%) patients had low calculated GFR (i.e., < 90 ml/min). Six patients had abnormal findings on routine and microscopic examination of the urine. Four (4.6%) patients had active sediment in the urine, 1 had nephrotic range proteinuria (i.e., ≥ 3.5 grams/day) and 1 patient had transient proteinuria. Kidney biopsy was done in only 4 patients (3 patients with active sediment in the urine and 1 patient with nephrotic range proteinuria) and kidney biopsy could not be done in the 5th patient because patient lost for follow up. Kidney biopsy of 1 patient with active sediment in the urine revealed membranoproliferative glomerulonephritis and 2nd patient revealed membranous nephropathy. Kidney biopsy of the 3rd patient with active sediment in the urine was inadequate for opinion and patient did not consented for the repeat biopsy. Kidney biopsy of the patient with nephrotic range proteinuria revealed membranous nephropathy. GFR was calculated for all patients using Cockcroft-Gault formula. GFR distribution of the patients is shown in [Table - 2]. Mean GFR in patients with diffuse SSc was 77.55±29.15 whereas mean GFR in patients with limited SSc was 72.04±24.70. The difference was not statistically significant ( P =0.67). Further analysis was carried out to see if the extent of the disease, duration of the disease, steroid and/or calcium channel blocker nifedipine intake had any relation with GFR [Table - 3]. Eighty patients (92%) were receiving nifedipine and sixty patients (69%) were receiving steroid therapy. None of the above mentioned parameters had significant influence on the GFR. Discussion The present study brings out some of the important features of SSc as seen in a tertiary care hospital in Northern India. Clinical features were comparable to the incidence stated in the western literature except calcinosis, telangiectasias and renal involvement.[11] This low incidence of calcinosis and telangiectsia is not entirely being explained by dark color skin of our population. Incidence of calcinosis may be underestimated as it was not assessed by means of imaging. There was no correlation found between the renal involvement and other organ involvement. Renal involvement in our population is of non-renal crisis type. Twenty six (~ 30%) of our patients had Chronic Kidney Disease by definition (i.e., GFR < 60 ml/min). GFR was calculated using Cokcorft-Gault formula in our study, which has been found to correlate well with GFR, which is measured using a radioisotope clearance method in a recent study by Kingdon et al .[12] None of our patients had SRC, which is reported in upto 15% patients with diffuse scleroderma in western population. It is difficult to explain the rarity of SRC in these patients only on the basis of early use of anti hypertensive drugs. We feel there may be selection bias in patient recruitment as study is conducted at single tertiary center. This finding is consistent with one early study from India by Desai et al .[5] Renal biopsy has revealed primary glomerulopathy in three patients - one membranoproliferative and two other membranous nephropathy, suggesting more of lupus or scleroderma overlap syndrome. But in these patients clinical picture, as well as serological profile does not suggest lupus or overlap syndrome. Significant renal disease occurs mostly in patients with diffuse cutaneous scleroderma.[13] We therefore compared the mean GFR in diffuse SSc patients with limited SSc patients. Mean calculated GFR in patients with diffuse scleroderma was 77.55 ± 29.15 as compared to 72.04 ± 24.70 and this difference between the two groups was statistically not significant ( P =0.67). Majority of SRC have been reported to occur during the first 4 years of the illness.[3] Therefore, we compared the mean GFR in patients with disease duration < 48 months and in those with 48 months. Patients with < 48 months of disease duration had higher (79.14 ± 30.17) mean GFR as compared to those with disease duration of > 48 months (72.00 ± 23.34), suggesting the decline of kidney function with duration of the illness. Prednisolone use has been reported to be an important predictor of SRC.[14] Therefore, we calculated the mean GFR in patients who were taking > 7.5 mg/day equivalent of prednisolone and those who were not taking. Mean GFR tended to be higher in the group with steroid intake (77.5 ± 30.43) than in the group without steroid intake (71.90 ± 19.55). This difference however was statistically not significant. As majority 92% of our patients were on nifedipine therapy for the treatment of Raynaud′s phenomenon, we thought that this might be providing nephroprotection because of its vasodilating effect on renal arterioles. Though the patients who were taking nifedipine had apparently higher mean GFR (76.50 ± 28.03) than those who were not taking (61.33 ± 16.44), the difference did not attain statistical significance ( P =0.46). However, these 2 groups were incomparable because of the small numbers of patients in the group without nifedipine therapy. The present study has few important limitations, the most important being cross sectional study it may not give us the exact cumulative frequency and details of renal involvement in Indian patients with SSc. We need to have larger sample size with long term follow up. The other important limitation of the present study is non-availability of kidney biopsy in all patients, which was not possible because of the ethical issues involved. Conclusions We conclude that SRC is very rare in Indian patients with SSc. However, nonrenal crisis abnormalities appear to be as common in Indian patients with SSc as compared to the western literature. We suggest that further studies needs to be done to find out the exact details of the renal involvement in Indian patients with SSc. Acknowledgement Dr. S. K. Agarwal, Additional Professor, Department of Nephrology, All India Institute of Medical Sciences, New Delhi - 110029 for their guidance and review of the manuscript. References
Copyright 2007 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms07015t3.jpg] [ms07015t2.jpg] [ms07015t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}