 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
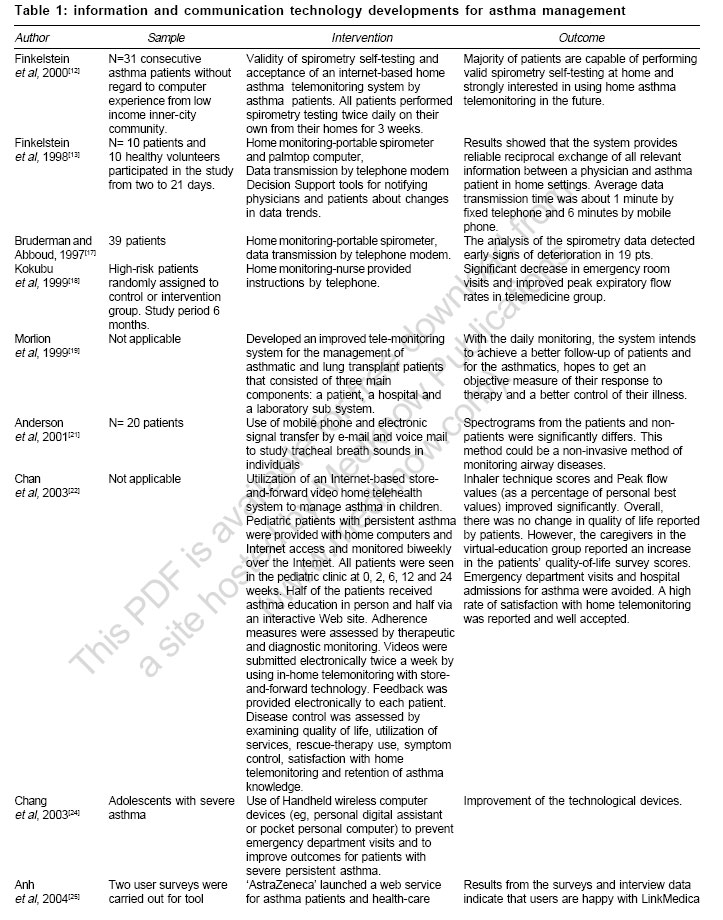
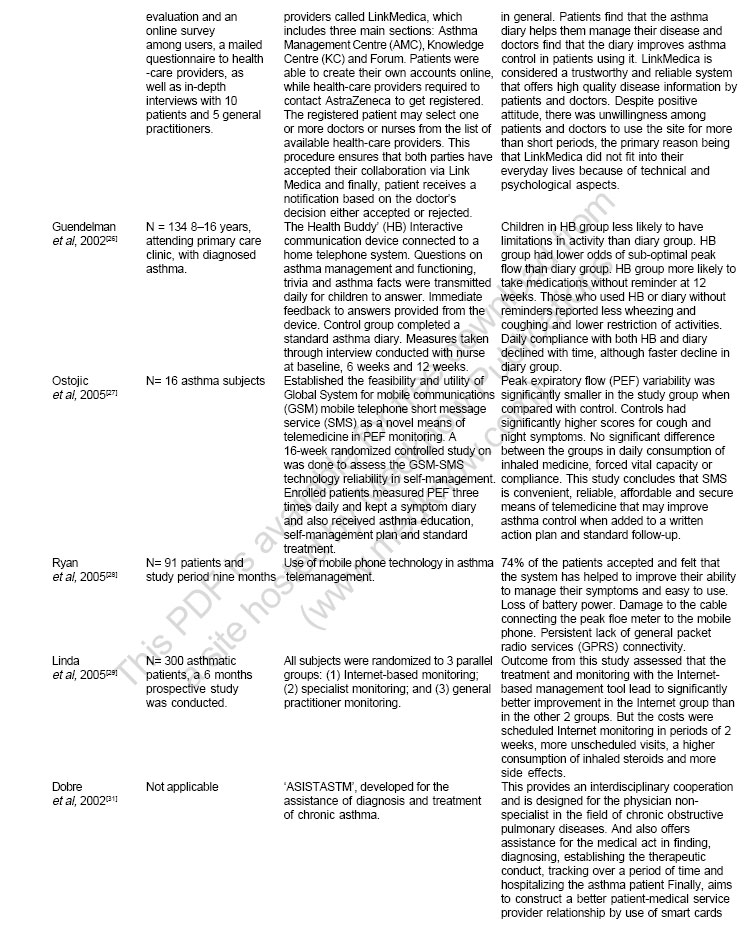
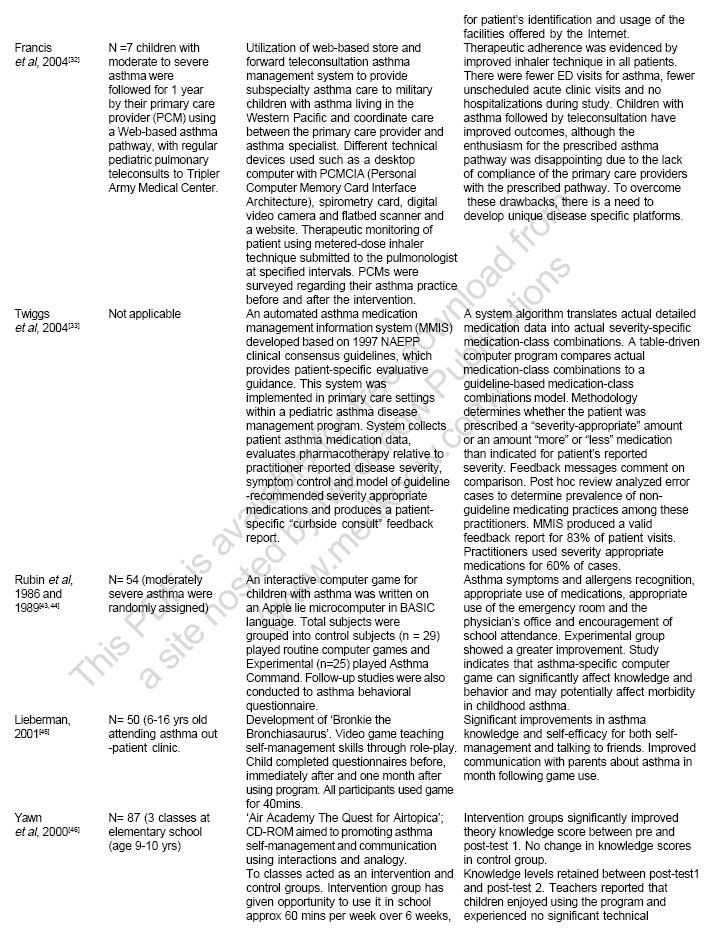
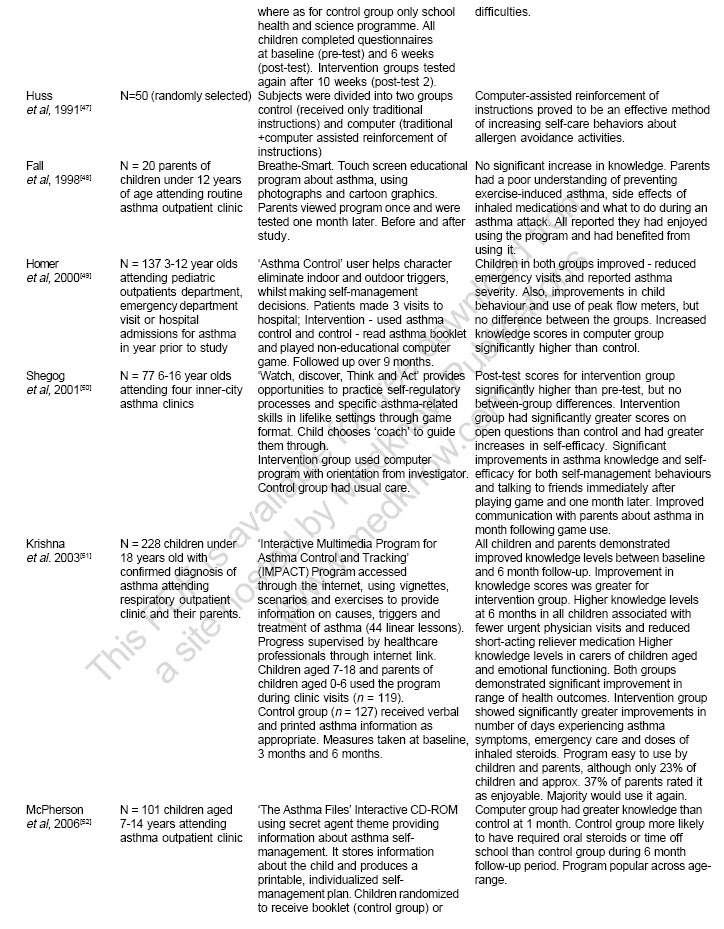
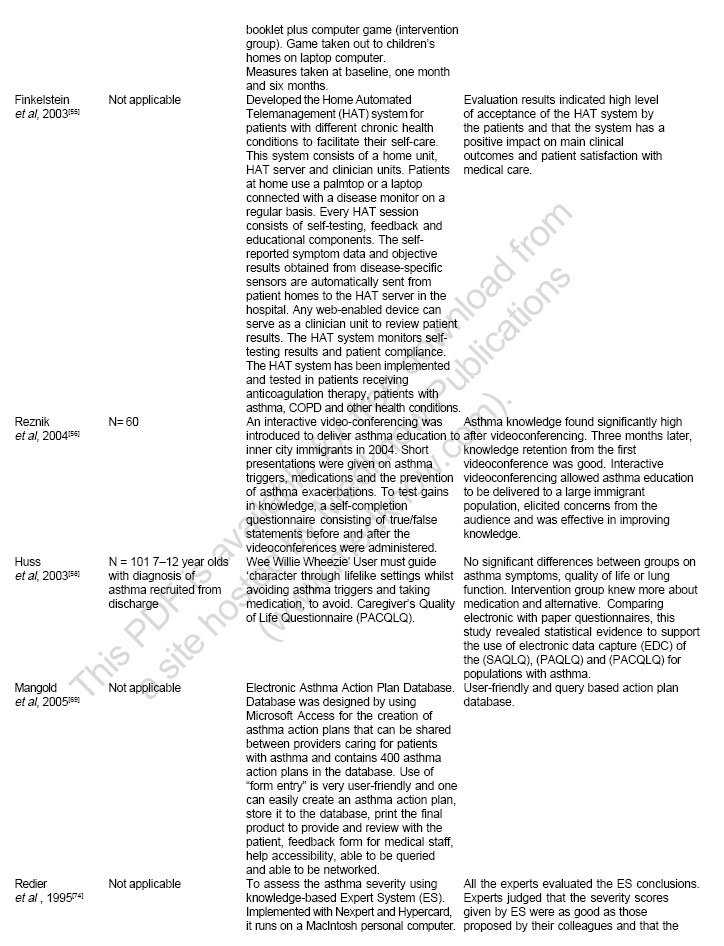
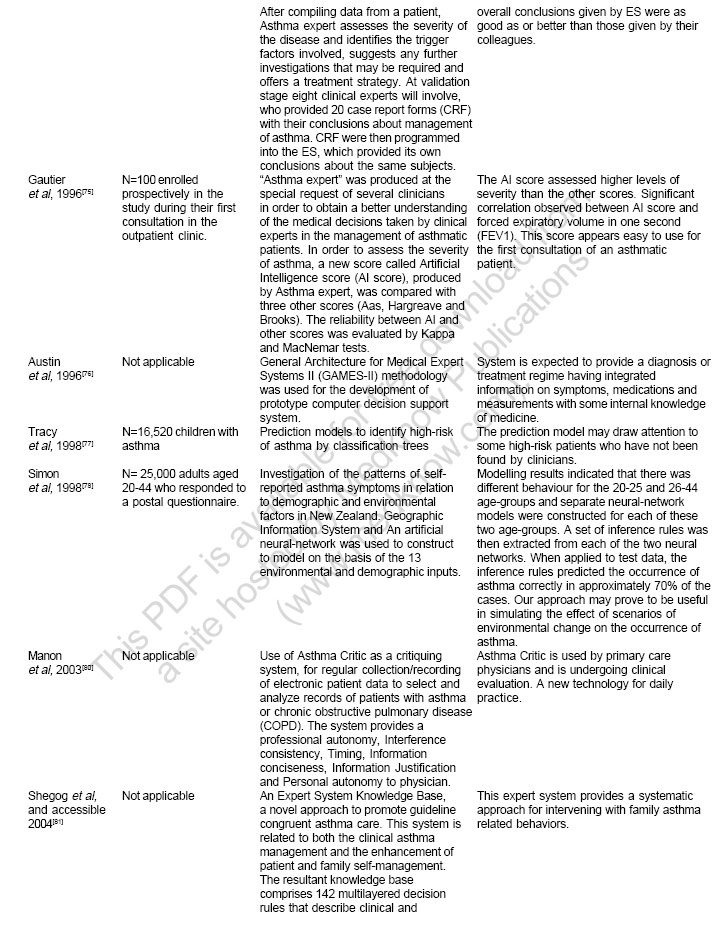
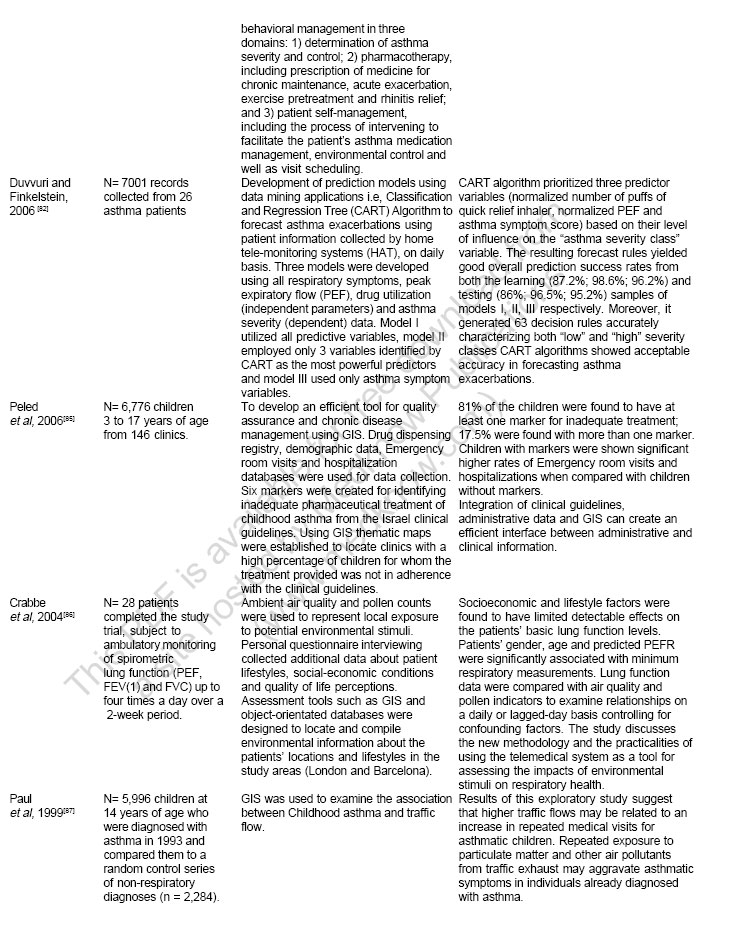
Indian Journal of Medical Sciences, Vol. 61, No. 4, April, 2007, pp. 221-241 Practitioners section Information and communication technology developments in asthma management: A systematic review Duvvuri Venkata RamaSatya Kumar, Jianhong Wu Department of Mathematics and Statistics, York University, Toronto, Ontario Code Number: ms07038 Abstract This review aims to explain the progress of information and communication technology (ICT) applications in asthma management. Appropriate literature was printed out from the bibliographic databases and library source using relevant key phrases of ICT and asthma. The ICT developments from simple to complex modules to augment the conventional methods of asthma care with a caution of excessive reliance upon technology were discussed. However, it should be noted ICTs are for maximizing the human clinician's own ability to receive and process information as well as providing unique opportunities for patients, physicians, pharmacists and researchers.Keywords: Asthma, communication, information, management, technology Background Asthma is an inflammatory chronic public health problem throughout the world [Figure - 1] affecting people of all ages, which can result in variable restriction in the physical, emotional and social aspects of a patient's life.[1],[2] It is estimated that around 300 million people in the world currently have asthma.[3] The prevalence of asthma increases as communities adopt modern lifestyles and become urbanized.[4] With the proportion of the world's population living in urban areas projected to increase from 45 to 59% in 2025, there is likely to be a marked increase in the number of people with asthma worldwide over the next two decades. It is estimated that there may be an additional 100 million people with asthma by 2025.[5] Effective management of chronic illness requires a close partnership between the patient and all health care providers.[6] Recent studies have shown that long-term monitoring of asthma severity can reduce asthma exacerbations, optimize drug therapy and decrease the cost of asthma management.[7] The management of a chronic patient is a collective and cooperative enterprise that may exploit Information Technologies to improve the overall quality of care.[8] Most consideration among them is given to Internet technologies and decision-support technologies.[9],[10],[11] Emerging at the beginning of the last decade, the world-wide web rapidly imposed itself as a new medium for interconnecting people throughout the world. Overstepping the initial publishing purpose, Web applications currently evolve towards the setting up of virtual working and communication spaces, intended to be used by specific communities of users.[12] The use of the web for telemedicine applications seems now-a-days a compulsory solution: the web has become a standardized infrastructure for giving access to sophisticated telemedicine applications from virtually any machine and operating system. Such standardized communication platform guarantees accessibility and usability advantages to both patients and physicians.[13],[14] The aim of this review is to emphasize the advancement of technological trends in asthma management that are significantly involved in every phase of telemanagement/remote management of chronic disease. This paper is structured as sections: 1. Background; 2 Materials and Methods; Materials and Methods We developed a search strategy to find any publications about the computer, communication and information technology related to asthma and used these to search the MEDLINE (1966 to current update), CINAHL, DOAJ, PubMed databases using the key phrases telemedicine, teleconsultation, telepharmacy, patient education, database, decision support system (includes artificial intelligence, decision trees, neural networks, expert system), geographical information system and asthma. The appropriate literature was printed out from the online source and library (journal) source.Results and discussion From the review of literature, we found some important cornerstones, which can play their indispensable role in effective management of asthma [Table - 1a, b, c, d, e, f, and g in pdf]. These were discussed in detail under the following sub-headings. Telemonitoring (TM) TM is defined as the use of information and communication technology (ICT) to monitor patients at a distance or for remote monitoring of patients, including the use of audio, video and other telecommunication and electronic information processing technologies.[15] In 1905, Dr. Einthoven transmitted electrocardiograms (ECGs) from hospital to his laboratory by directly connecting immersion electrodes to remote galvanometer via telephone lines.[16] Patients with asthma have been telemonitored with digital spirometry devices, as have cardiac with pacemaker and ECG monitoring.[17] Various research groups have exploited the date-to-date advancements in ICT for TM of asthma, thereby, leading to the improvement of disease management. Kokubu et al.[18] developed a telemedicine system to monitor the airway status at home for patients with poorly controlled asthma, whereby a nurse, under the supervision of their physicians, provides instructions to individuals via the telephone to help them manage exacerbation. The number of emergency room visits decreased significantly and the activities of daily living improved in the telemedicine group. Home TM system was developed for improved management of asthmatic and lung transplant patients, with daily monitoring and better follow-up.[19],[20] These systems allow early recognition of potentially dangerous situations and timely interventions. A telematic system for monitoring of asthma severity in patients' homes was developed by Finkelstein et al. to deal with these limiting factors.[13] Results showed that the system provides reliable reciprocal exchange of all relevant information between a physician and patient in home settings. A follow-up study was done by same group[12] to evaluate the validity of spirometry self-testing and to assess the acceptance of an Internet-based home asthma TM system by patients. Majority of patients indicated that the self-testing was 'not complicated at all' and also showed strong interest in using home asthma telemonitoring in the future. Anderson et al.[21] used mobile phone and electronic signal transfer by e-mail and voice mail to study tracheal breath sounds, which are widely accepted as an indicator of disease activity in patients. Spectrograms from patients were significantly different from those from people without asthma. The immediate benefit of mobile phone recordings includes accurate timing of the measurement, which might for instance improve compliance with an associated peak flow measurement. For the first time, a web-based home monitoring integrated store-and-forward video technology was developed by Chan et al . to improve the adherence to medications, especially those requiring careful technique.[22] There was high rate of satisfaction with home TM, followed by no emergency department visits, hospitalizations and few unscheduled visits. Handheld wireless computer devices such as Personal Digital Assistance (PDA) were used to facilitate data transfers and frequent communications between the nurse and the adolescent asthmatic patient.[24] Usage of PDA resulted in obtaining information about patients' behavior and maintaining patients' behavior to control their asthma on a regular-basis, which ultimately increased the quality of life. PDA technology cost will be less than the cost of emergency department visits ($1,324 per patient) or inpatient hospital stays ($5,316 per patient).[23] In May 2000, AstraZeneca launched a Web service called LinkMedica for asthma patients and health-care providers.[25] Patients found asthma diary helps them to manage their disease, and doctors found that the diary improves asthma control in patients using it. But there was unwillingness among patients and doctors to use the site for more than short periods, the primary reason being that LinkMedica did not fit into their everyday lives due to technical and psychological aspects. Similar to LinkMedica, another program, the Health Buddy (Health Hero Network), was designed.[26] Ostojic et al.[27] established the feasibility and utility of Global System for mobile communications (GSM) mobile telephone short message service (SMS) for PEF monitoring. The results concluded that SMS is a convenient, reliable, affordable and secure means that may improve asthma control. Mobile phone technology was used in asthma telemanagement by Ryan et al.[28] to assess patient compliance. The primary outcome measure was compliance. Despite positive results, some technical difficulties were observed. A study was conducted to assess the outcome of monitoring and treatment using a physician-managed online interactive asthma monitoring tool, which comprises three modules: an electronic diary, an action plan for the patients and a decision support system for the physician, in comparison with conventional asthma treatment by Linda et al .[29] The outcome was significantly improved quality of life, lung function and airway responsiveness for the Internet group, but the costs were scheduled Internet monitoring in periods of 2 weeks, more unscheduled visits, a higher consumption of inhaled steroids and more side effects. Above-mentioned TM allows the patient to monitor his or her disease severity continuously in natural environment, which avoids the 'white-coat' effect and allows the physician to obtain a more realistic view of the patient's health status on a day-to-day basis. The main setbacks of TM development include the initial costs of systems, physician licensing and reimbursement. Teleconsultation (TC) The use of ICT is to enable clinical consultation between geographically separated individuals, such as health care professionals and their patients.[30] TC is the deliberation by two or more physicians with respect to diagnosis or treatment in a particular case via ICT. Often, it involves the process of obtaining an opinion from a specialist, where there is no consideration payable to the specialist assuming care for the patient. Telemedicine lends itself readily to the process of consultation. It may allow a venue for patient referral and, in many cases, will help to avoid or at least facilitate patient transfer. ASISTASTM is a system developed for the telematic assistance in diagnosis and treatment of chronic asthma.[31] The system offers assistance for the medical act in finding, diagnosing, establishing the therapeutic conduct and tracking over a period of time by use of smart cards for patient's identification and usage of the facilities offered by the Internet. Francis et al.[32] implemented a web-based store-and-forward teleconsultation asthma management system to coordinate care between the primary care provider and asthma specialist. In this study, different technical devices were used, such as a desktop computer with Personal Computer Memory Card Interface Architecture, spirometry card, digital video camera and flatbed scanner (for radiographs) and a website. No patients were hospitalized during study, and the provision of asthma education increased from 18 to 73%. Children with asthma followed by TC have improved outcomes, although the enthusiasm for the prescribed asthma pathway was disappointing due to the lack of compliance of the primary care providers with the prescribed pathway. To overcome these drawbacks, there is a need to develop unique disease-specific platforms. Twiggs et al.[33] developed an automated asthma medication management information system that provides pediatric asthma disease management program. Post hoc review analyzed error cases to determine prevalence of nonguideline medicating practices among these practitioners. Practitioners used severity-appropriate medications for 60% of cases. Patient Education (PE) Communication between the patient and the family physician is a key factor affecting both the process and outcome of care. Well-informed patients are more likely to become active partners in the management of their own health.[34],[35],[36] According to the Diagnosis and Management of Asthma Expert Guidelines,[37] PE is a critical component of quality asthma care.[38] a. Pediatric and adolescent asthma education: Various researchers have developed interactive computerized PE programs and concluded that they are effective in the management of several diseases.[39],[40],[41],[42] Asthma command program showed improvements in knowledge and in self-reported asthma management in patients, when compared with children in the control group.[43],[44] Bronkie the Bronchiasaurus has been shown to positively affect knowledge, self-efficacy and communication about asthma in children who use it.[45] Airtopia has been shown to positively affect asthma knowledge in children when used in the context of a general health curriculum,[46] and gained knowledge was retained over a 4-week period. However, in the above studies there were no demonstrated differences in visits to physician, emergency rooms or hospitals. To determine computer-assisted instruction effects on adherence to implementing house dust mite avoidance measures in adult atopic asthmatics, Huss et al.[47] conducted a randomized study. Results have indicated significantly greater adherence scores to computer group when compared to other. Another interesting education program 'Breathe-Smart,' a touch screen using photographs and cartoon graphics, was developed by Fall et al. ,[48] but they found much encouraging outcomes. Homer et al.[49] created 'Asthma Control,' which helps to improve children's behavior in terms of protecting from indoor and outdoor triggers. This program was found to be considerably useful for making self-management decisions. Shegog et al.[50] developed a pediatric asthma self-management education program 'Watch, Discover, Think and Act.' Evaluation reports demonstrated significant higher scores and improved self-efficacy. Chan et al.[22] developed for the first time a web-based integrated store-and-forward video technology to test the feasibility and effectiveness of Internet-based asthma education. A handheld communication device such as PDA was used to improve the outcomes of adolescent patients with severe persistent asthma.[24] Guendelman et al.[26] reported that educational interventions through an integrated self-management educational program Health Buddy (Health Hero Network) encouraged children's active involvement in the control of their asthma problems. Krishna et al.[51] developed an 'Interactive Multimedia Program for Asthma Control and Tracking' to access the information on causes, triggers and treatment of asthma through an Internet. An improvement of knowledge levels, fewer urgent physician visits and reduced medication were observed. Very recently, McPherson et al.[52] established an Interactive CD-ROM using 'secret agent' theme providing self-management information, and outcomes revealed that intervention group gained greater knowledge. Most of the studies have reported similar findings when evaluating educational programs for children, most notably higher knowledge levels, although the method and content vary between studies. Positive effects upon clinical outcomes have been demonstrated in some studies. b. Adult asthma education: For adult asthma patients, computer-assisted instructions (CAI) have been used to help them monitor and avoid house dust and/or mite allergen.[53] Two asthma studies evaluated instructional computer programs to educate patients about allergen-avoidance activities.[53],[54] Takabayashi et al.[54] studied the effect of asthma educational software for computer-assisted instruction. Emergency visits or admissions at least 1 year after the first CAI trial decreased. Finkelstein et al.[55] developed the Home Automated Telemanagement (HAT) system and indicated high level of acceptance by the patients and that the system had a positive clinical impact and patient satisfaction. An interactive video-conferencing was introduced to deliver asthma education,[56] and participants gained significant asthma knowledge. Interactive video-conferencing allowed asthma education to be delivered to a large immigrant population, elicited concerns from the audience and was effective in improving knowledge. Despite benefits, there are a few considerable drawbacks of using computer technology for health education, such as lower socioeconomic groups,[57] lack of technology availability, lack of literacy skills and algorithm complexity.[58] Future computer interventions must be evidence based, and detailed evaluation work is essential. Telepharmacy (TP) Pharmacy is a knowledge profession built on the collection, evaluation, communication and use of drugs, diseases and patient information. In 1997, the National Association of Boards of Pharmacy officially defined TP as 'the provision of pharmaceutical care through the use of telecommunications and information technologies to patients at a distance.'[59] According to Trottman, New York State Board of Pharmacy approved a regulation allowing prescriptions to be e-mailed over the Internet.[60] There is an urgent need to improve patient awareness about pharmacotherapy /drug usage by using system approaches, viz., 'TP,' to enhance pharmacy care that might be an effective way to reduce inappropriate medication use.[61] Providing instructions for correct MDI technique to patients can have a significant impact on asthma care.[62] Pharmacists are valuable members of health care teams, especially for patients of communities residing in areas where there is shortage of rural health professionals; such patients require consistent, reliable and readily available counseling services for chronic disease management.[63] Various communication systems that function as medication reminder aids may be useful. Monane et al.[64] conducted a study to evaluate whether a computerized drug utilization review database linked to a TP intervention can improve suboptimal medication use in the elderly. Using a system integrating computers, pharmacists and physicians, large-scale intervention improved prescribing patterns and quality of care. Steven et al.[65] used a 'Paging System' to improve medication self-management in asthmatic patients. Bynum et al.[62] conducted a study to determine the effectiveness of pharmacists using interactive compressed video in teaching MDI technique and patient satisfaction among adolescents with asthma. Both TP counseling and control groups participated in pre-, post-tests. Results demonstrated that patient education provided by pharmacists via interactive compressed video was superior to written instructions. Interactive compressed video is an effective medium for teaching and improving the critical health-related educational services to patients, including proper administration and dosages of drugs. These evaluation studies concluded that ICT is a potential intervention tool available to pharmacists in asthma care. The reviewed literature supports the use of ICT in pharmacy. Future research should focus on the demonstration of enhanced health outcomes resulting from improved prescribing choices. Databases and other information systems For any control program, baseline information in the form of systematic database is a primary requisite. The inter-relationships of the parameters can be studied through Database Management System. Collecting, storing, processing, managing and distributing information on all disease aspects can enhance efficiency in reducing asthma morbidity. In asthma management, several workers have developed various databases.[66] Molly et al.[67] used medication-dispensing information or prescription database from a large health maintenance organization to examine the utilization of anti-asthma medications. Results demonstrated the feasibility of using an automated outpatient pharmacy database to identify patients with asthma. Bushnell et al.[68] studied the utilization of electronic and paper administration of the standardized, pediatric and pediatric asthma caregiver's quality of life questionnaires. This study revealed statistical evidence to support the use of electronic data capture for populations with asthma. A user-friendly asthma action plan database was created for physicians and care providers to assist their adult asthma patients.[69] The use of 'form entry' is very user friendly, and one can easily create an asthma action plan, store it to the database, print the final product to provide and review with the patient; feedback form for medical staff; and help accessibility, able to be queried and able to be networked. Apart from the individual and community level applications, Thomas and Matthias[70] constructed an online resource for access to data on the genetics of asthma and allergy. Decision support systems (DSS) Artificial intelligence (AI) is the area of computer science focusing on creating machines that can engage on behaviors that humans consider intelligent. AI has split into several different approaches based on the opinions about the most promising methods and theories. DSS is a computer application designed to aid clinicians in making diagnostic and therapeutic decisions in patient care. Clinical practice guidelines have been written to stipulate recommendations for the appropriate delivery of care in specific clinical situations.[71] These guidelines have little impact upon actual clinical practice unless they are effectively integrated into the clinical setting.[72] Hence, there is an urgent need to utilize ICT, which can facilitate the use of electronic medical records, Computer-based DSS could be used to integrate practice guidelines into the process of health care delivery.[72],[73] Asthmaexpert, a Knowledge-based Expert System to assess asthma severity, has been developed by Redier et al .[74] It has been critically evaluated by the clinical experts and identified as a useful tool for discussing the management of asthma.[75] During 1996, Austin et al.[76] developed a prototype Computer DSS based on their General Architecture for Medical Expert Systems II methodology. This system is expected to provide a diagnosis or treatment regime having integrated information on symptoms, medications and measurements, with some internal knowledge of medicine. Computer-based prediction models were developed by Tracy et al.,[77] who concluded that these models can identify asthmatic children at high risk for future hospitalization and emergency department visits and may direct attention towards some high-risk patients who have not been found by clinicians. Simon et al.[78] investigated the role of demographic and environmental factors in patterns of adult asthma symptom prevalence using connectionist-based analysis. Juan et al.[79] employed algorithm proposed by Panhuysen and co-workers approach for the diagnosis of asthma in Chinese population with a high prevalence of smoking, as well as in an inability to explore any potential interactions between the genetic factors and cigarette smoking in the pathogenesis of asthma. From this study, they found that there is no correlation between the asthma and mapping genes that contribute to asthma, because these objects may be influenced by a smaller number of genes. Asthma Critic is a non-inquisitive critiquing system that generates critiquing comments and adds these comments to the patient record. This system uses routinely recorded electronic patient data to select and analyze records of asthma and chronic obstructive pulmonary diseases.[80] Shegog et al.[81] developed an Expert System Knowledge Base to promote guideline-congruent asthma care. This tool comprises 142 multilayered decision rules, which provide a systematic and accessible approach for intervening in family-asthma-related behaviors. Recent studies by Duvvuri and Finkelstein[82] employed AI applications, viz., Classification and Regression Tree Algorithm, to forecast asthma exacerbations using patient information collected by HAT, on daily basis. This asthma DSS intends to aid the physician in prioritizing asthma-triggering parameters and to predict the asthma severity zone. These are the works that highlight the usefulness of DSS, but a number of short-term and long-term risks are inherent in the use of such systems, however. The most immediate risks are those associated with the reliability and integrity of the software itself. Only properly trained health professionals know when to rely on such system and how to use the rules/output generated from such systems. Geographical information system (GIS) Epidemiological data from all over the world show an increasing prevalence of asthma morbidity and mortality despite the availability of effective treatment and also large geographic variations in asthma outcomes.[83] These facts led to the emergence of strategies developed to improve the quality of asthma care. The use of information technologies such as GIS has great potential for the management of chronic disease. GIS refers to computer-based programs with five basic functional components: 1. Acquisition and verification of data, 2. Data storage and database management, 3. Transformation and Analysis of data, 4. Data Visualization and 5. User Interface.[84] One of the more powerful features of GIS is the ability to link several databases such as demographic, clinical and billing systems and create a high-resolution demonstration of the spatial distribution and or behavior of the phenomenon. Therefore, the use of GIS in health-related studies is emerging as an important tool in health care planning, quality assurance and research. Several studies for asthma disease management were conducted using GIS approach, such as thematic maps to locate the clinics with percentage of children for whom the treatment provided was not in adherence with the clinical guidelines.[85] These maps demonstrated in a robust way the association between inappropriate treatment and adverse effect. As an outcome, an efficient tool based on GIS approach was developed for allocating sites for quality assurance interventions. In a study to examine the effect of pollutants and allergens on asthmatic respiratory health, GIS with object-oriented databases were designed to accurately locate and compile environmental information about the patient's location and lifestyles in study areas.[86] In a case-control study, GIS was used to examine the association between childhood asthma and traffic flow. GIS allowed quick linkage of traffic count information to geocoded (ability to locate residences in space) address of asthma patients. The exploratory study suggested that high traffic flows might be related to an increase in repeated medical visits by asthmatic children due to exposure to pollutants.[87] The integrative features of modern GIS technology are incredibly helpful in summarizing the complex relationships between chronic diseases and environment and human population. Conclusions Rapid technological advances have prompted the development of a wide range of telemanagement systems to enable the prevention, early diagnosis and management of chronic conditions. The Internet age is altering the patient-physician relationship. Through the understanding of evolving professional roles, the decision-making process among physicians and patients may improve with efforts to share the burden of responsibility for knowledge. This change could usher in a new era of patient-physician relationship, with a potential gain for all collaborative parties. The challenge is to leverage the opportunity of shifting home telemedicine technology from provider-focused to patient-focused healthcare delivery. As a population and providers of health care, we are in the infancy stages of this approach. There are many questions to be answered. There are many challenges - technical, professional and interpersonal. But from all preliminary indications, patients have embraced this approach, both clinically and economically. Those patients who currently feel that the health care delivery system is reducing their health care benefit may achieve a whole new level of access and satisfaction with a home tele-health-based disease management approach.References
Copyright 2007 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms07038t1g.jpg] [ms07038f1.jpg] [ms07038t1f.jpg] [ms07038t1d.jpg] [ms07038t1b.jpg] [ms07038t1e.jpg] [ms07038t1a.jpg] [ms07038t1c.jpg] |
| |||||||||

![[Figure - 1]](/showimage?ms/photo/ms07038f1.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}