 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
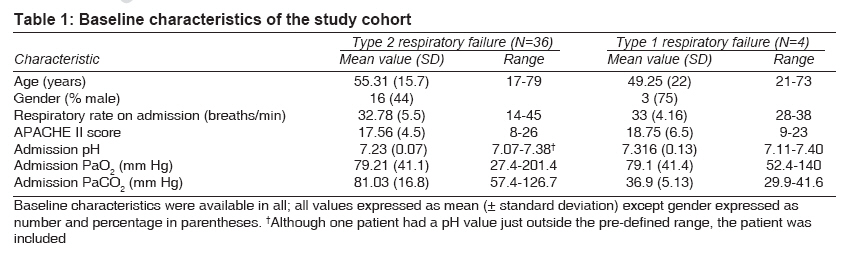
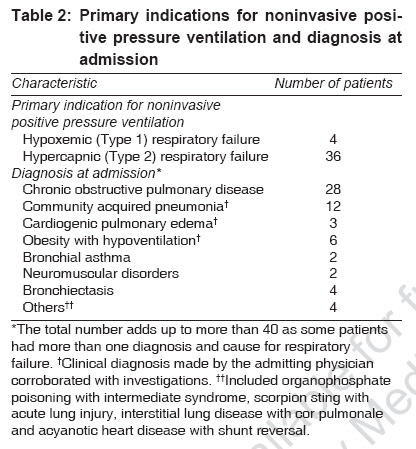
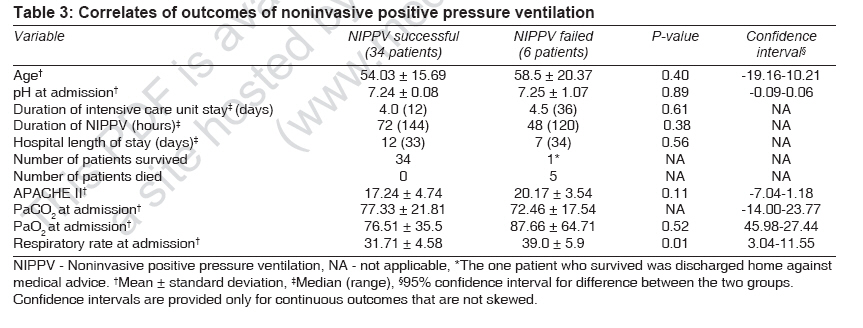
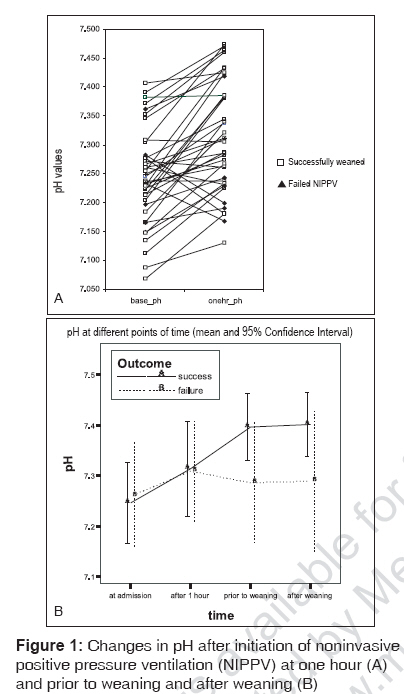
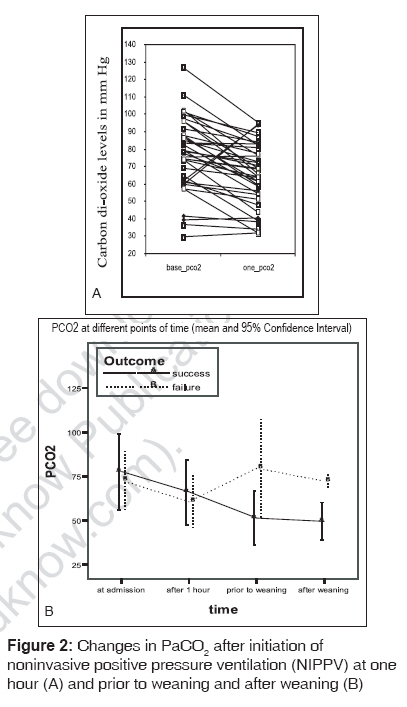
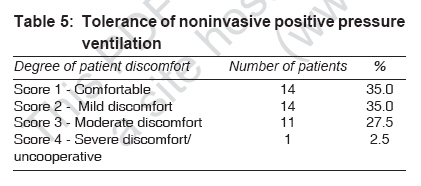
Indian Journal of Medical Sciences, Vol. 61, No. 9, September, 2007, pp. 495-504 Original Contributions An evaluation of the role of noninvasive positive pressure ventilation in the management of acute respiratory failure in a developing country George IgeAbraham, John George, John Preeta, Peter JohnVictor, Christopher Solomon Department of Medicine, Christian Medical College and Hospital, Vellore Code Number: ms07081 Abstract Objective: Noninvasive positive pressure ventilation (NIPPV) has been shown to decrease the need for invasive mechanical ventilation (MV) in patients presenting with acute respiratory failure (ARF). We conducted a prospective study to assess if NIPPV use, in a developing country, was associated with clinical and physiological improvements.Design: Prospective observational study. Materials and Methods: Forty patients admitted to a medical intensive care unit during a 2-year period who fulfilled criteria for inclusion formed the study cohort to receive NIPPV. Findings: Baseline (mean ± SD) pH, PaCO 2 and PaO 2 were 7.25 ± 0.08, 76.6 ± 20.9 and 79.18 ± 40.56 mmHg respectively. The primary indication for NIPPV was hypercapnic respiratory failure (n = 36, 90%). The success rate with NIPPV was 85%, with 34 of 40 patients weaned successfully. Significant improvements were observed at 1 hour following institution of NIPPV in pH (7.31 ± 0.09, P < 0.001) and PaCO 2 (65 ± 17.9, P < 0.001). These improvements continued up to the time of weaning (pH 7.38 ± 0.08, PaCO 2 54.7 ± 20) and maintained (within 12 h) postweaning from the ventilator (pH 7.39 ± 0.08, PaCO 2 51.9 ± 12.4). No significant change in the PaO 2 was observed during NIPPV; PaO 2 after 1 h, prior to weaning and after weaning was 90.53 ± 42.85, 84.80 ± 33.76, 78.71 ± 43.81 respectively. Conclusion: This study has demonstrated benefits of NIPPV in avoiding the need for invasive MV in patients presenting with ARF of diverse etiology, with results comparable to developed nations. Increased use of NIPPV in ARF is likely to impact favorably in nations with limited resources. Keywords: Acute respiratory failure, chronic obstructive pulmonary disease, noninvasive positive pressure ventilation, outcomes The recent critical-care literature has seen an explosion of articles on noninvasive respiratory support for patients presenting to hospital with respiratory failure of diverse etiology, with numerous published randomized controlled trials (RCTs) and meta-analyses on this topic. [1],[2],[3],[4],[5] Although this subject has been widely researched in the developed world, there is still a paucity of literature in the developing nations, where this modality of treatment assumes greater relevance, given the limitations of resources. If such treatments could be successful in reducing the requirements of invasive mechanical ventilation (MV) in patients with respiratory failure, it could have a potentially favorable impact on the allocation of the sparse health resources to other reversible causes of respiratory failure. Two recent publications from India suggested that noninvasive positive pressure ventilation (NIPPV) was beneficial in cohorts of patients presenting with chronic obstructive pulmonary disease (COPD), as well as respiratory failure of varied etiology. [6],[7] This prospective study was undertaken to assess the feasibility of use of NIPPV and to ascertain its role in a medical intensive care unit (MICU) in a developing country. The primary aim of this study was to evaluate if NIPPV was associated with a reduction in the need for invasive mechanical ventilation and to ascertain if it resulted in successful weaning from NIPPV in patients presenting with acute respiratory failure (ARF) of diverse etiology. In addition, improvements in physiological parameters (improvements in pH and PaCO 2 ) were also assessed and recorded. Materials and Methods In this prospective observational study, all patients admitted to the medical ICU of a tertiary referral university-affiliated hospital in south India during the period September 2002 to February 2004 were evaluated for feasibility for NIPPV. Patients were eligible for entry to the study if they presented with ARF without a clinically perceived need for immediate life-saving endotracheal intubation (i.e., patients with severe hypoxemia and impending respiratory arrest requiring immediate endotracheal intubation were ineligible). This study was approved by the hospital′s Ethics and Research Committee. ARF was defined as (a) acute respiratory failure, evidenced by tachypnea (>24 breaths/min), and arterial pH < 7.32 and/or PaCO 2 > 38 mmHg; or (b) hypoxemic respiratory failure evidenced by severe tachypnea (>24 breaths/min) with gas exchange derangements (PaO 2 < 60 mmHg or ratio of PaO 2 to FiO 2 ≤200 mmHg on room air) after an aggressive and appropriate medical therapy including oxygen supplementation. [8] Patients were excluded from the study if they (a) were not candidates for endotracheal intubation because of a ′do not resuscitate′ order (although this did not preclude the use of NIPPV outside the study); (b) needed airway protection because of altered conscious state (GCS < 8) or copious respiratory secretions that they could not clear easily; (c) were unable to tolerate NIPPV due to extreme claustrophobia or anxiety despite repeated attempts to facilitate the use of NIPPV; (d) had severe acidosis (arterial pH < 7.10) or (e) presented with shock (either cardiogenic or septic) with a systolic blood pressure of < 90 mmHg despite fluid challenge or need for pressor agents. Patients presenting with respiratory failure related to an acute coronary syndrome were also not included in the study as they were managed at the coronary care unit and not the MICU. Once eligibility for the study was verified, informed consent was obtained either from the patient or from his/her closest relative. Patients were initiated on bi-level positive airway pressure support using the BiPAP ® S/T-D Ventilatory Support System (Respironics, Inc.) and a face mask (′Performatrak′ from Respironics, Inc.). Inspiratory positive airway pressure (IPAP) was initially set at 10 cm H 2 O and increased by increments of 5 cm of H 2 0 up to 25 cm H 2 O based on clinical response and arterial blood gases. The initial expiratory positive airway pressure (EPAP) was set at 5 cm H 2 O and was not altered unless clinically indicated. The need for subsequent changes in IPAP and EPAP, as well as decision for supplemental oxygen, was determined by the intensivist. Additional humidification was not provided with these machines. Patients were monitored based on clinical parameters, pulse oximetry and arterial blood gases. On initiation of NIPPV, continuous application was encouraged. Supplemental oxygen therapy was administered with NIPPV and titrated to achieve a saturation of 88-92% unless clinically determined otherwise. Oximetry was correlated with arterial blood gas analysis at the end of 1 h of application of NIPPV and at subsequent intervals determined by the treating physician. Previous studies have suggested that clinical and oximetric improvements at 1 h portend a favorable response. [9],[10] On this basis, if there were clinical and/or laboratory evidence of deterioration at the end of 1 h or subsequently, endotracheal intubation was considered. Bronchodilators were administered as nebulisers where clinically indicated. Once the patient improved clinically and corroborated by improvements in arterial blood gases, weaning was initiated. During the weaning phase, the IPAP was decreased in gradations of 2-3 cm till the IPAP was 7-10 cm. The application was then switched over to intermittent use, and the duration of time off the NIPPV was determined by the treating physician. Weaning failure was defined as need for invasive mechanical ventilation or inability to wean the patient off NIPPV. Inability to wean the patient was either due to clinical features such as respiratory distress (tachypnea, tachycardia, increased work of breathing) or laboratory evidence of worsening or persistent respiratory distress while on NIPPV. The primary outcome measure in this study was the need for endotracheal intubation due to both early NIPPV failure (i.e., lack of response after 1 h of treatment) and NIPPV weaning failure or successful weaning from the NIPPV. Secondary outcomes included changes in arterial blood gas (ABG) parameters, hospital mortality, duration of ICU and hospital stay and complications (pneumonia and barotrauma). Pneumon--ia was defined as the appearance of new or progressive pulmonary infiltrates on a chest radiograph, associated with purulent tracheobronchial secretions, fever and peripheral blood leucocytosis. Microbiological confirmation was limited in several patients who were on NIPPV because of inability to obtain samples from the lower respiratory tract by bronchoscopy. Barotrauma was defined as the presence of air in the extra-alveolar spaces such as pneumothorax or pneumomediastinum, due to local over-inflation caused by high distending pressure. Patient comfort on the NIPPV was evaluated on a 4-point scale (scores 1-4). A score of 1 indicated that the patient was comfortable and cooperative; and a score of 2, slight discomfort with the patient still cooperative. Moderate discomfort associated with mild skin bruises, asynchrony, ill-fitting mask or claustrophobia but with the patient cooperative at most times was scored 3, whilst a score of 4 indicated severe discomfort in an uncooperative patient and the presence of skin necrosis or pressure sores and frequent disconnection from the ventilator. Statistical analysis was performed using SPSS software version 12. Parametric (t-test) or nonparametric (Mann-Whitney) was applied to continuous variables depending on normal or non-normal distribution. Categorical variables such as disease subgroups, types of respiratory failure and mortality were analyzed using the Fisher′s exact test owing to small expected frequencies. Results A total of 685 patients admitted to the medical ICU during the period September 2002 to February 2004 were evaluated for feasibility of NIPPV. Of the 40 patients fulfilling criteria for inclusion and initiated on NIPPV, 36 patients presented with hypercapnic respiratory failure. The study cohort [Table - 1] had a slight female preponderance (21:19) with a mean (SD) age of 54.7 (16.3) years and mean (SD) APACHE II score of 17.7 (4.5). Common diagnoses included COPD exacerbation and community-acquired pneumonia [Table - 2]. The success rate with NIPPV was 85%, with 34 patients weaned successfully off noninvasive ventilation. Failure rates were similar ( P = 0.57) in the hypercapnic respiratory failure group (5/36, 14%) and the hypoxemic respiratory failure group (1/4, 25%). Of the 6 patients who failed NIPPV, 3 patients were not intubated because of a conscious decision not to escalate therapy; the decision was taken subsequent to recruitment to the trial after discussing prognosis and further treatment options with the relatives. One of these 3 patients was discharged against medical advice (he had atrial septal defect with shunt reversal and COPD), whilst the other 2 patients expired while on NIPPV (both were COPD patients aged> 60 years and had directives not to escalate therapy beyond NIPPV). The other 3 patients who failed NIPPV were intubated and mechanically ventilated. All these 3 patients also eventually succumbed - 2 due to severe ventilator-associated pneumonia and 1 from gram-negative sepsis of urinary source. Although the APACHE II scores of the patients who failed NIPPV were higher (20.2) than those who were successful (17.2), this did not reach statistical significance ( P = 0.11). Respiratory rate at admission was significantly higher in the patients who failed NIPPV ( P = 0.01). No other differences were observed in baseline characteristics of patients who failed NIPPV versus those who succeeded [Table - 3]. NIPPV was used for a mean (SD) period of 82.8 (43.9) hours [Table - 3]. NIPPV was associated with significant improvements in pH and PaCO 2 [Figure - 1], [Figure - 2] at 1 hour. These Improvements continued up to weaning and maintained postweaning from noninvasive ventilation [Table - 4]. There was no significant change in the PaO 2 during NIPPV. NIPPV was well tolerated [Table - 5], with only 30% experiencing significant discomfort. This was managed with frequent reassurance to the patient, added skin care (application of oil, padding) and the use of very small doses of sedation (midazolam or haloperidol). The most common problem faced with NIPPV was air leaks seen in a third of the patients (14/40). This was due to ill-fitting masks; and with the use of appropriately sized mask, it was minimized. Mild skin bruising occurred in 4 patients (10%) whilst skin necrosis and pressure sores developed in 3 patients who were on long-term steroids (7.5%). In these 3 patients, these occurred during the weaning phase and were managed with ′cushion′ pads and use of a mask of appropriate size and by avoiding placing the head straps too tightly. Nosocomial pneumonias were diagnosed in 3 patients (7.5%). None had other complications of mechanical ventilation like barotrauma in the study cohort. Discussion The recent increase in the use of noninvasive ventilation in the acute care setting has been fueled by the desire to reduce complications of invasive ventilation and to improve resource utilization. The use of NIPPV in the management of acute exacerbations of COPD, as well as ARF of other etiology, is now supported by randomized controlled trials and meta-analyses. [1],[2],[3],[4],[5],[11] In these studies, NIPPV was associated with a reduced need for invasive MV, [1],[3],[4],[5],[11] decreased mortality [2],[3],[4],[5],[11] and shorter length of hospital stay. [3] Within the constraints of a prospective observational study, we report a good success rate for NIPPV using BiPAP ® . NIPPV was successful in 85% of patients in our study cohort. These results are consistent with previously published studies reporting success rates of 50-80% with NIPPV for ARF. [1],[2],[3],[4],[5] It is interesting to note that hypercapnic patients formed a significant (90%, n = 36) proportion of patients in our study. Of these, 28 patients were diagnosed to have COPD based on history, examination findings and pulmonary function tests. High success has been described with NIPPV in previous studies of patients presenting with hypercapnic respiratory failure. Brochard et al., in a similar group of hypercapnic patients with a mean baseline PaCO2 of 70 mmHg, observed a success rate of 74% (32/43) with NIPPV. [1]- In a subsequent randomized prospective study of NIPPV in ARF of varied etiology, Martin and colleagues reported a success rate of 78% in the subgroup of hypercapnic patients (n = 32). [8] Again the patients in this study had baseline characteristics similar to those of our patients. Plant and colleagues in a large trial of patients admitted with COPD exacerbation, again, showed that NIPPV was beneficial in reducing costs and improving outcomes. [2] However, this study was different from the above studies in that the patients were managed outside the ICU environment. It was difficult to draw meaningful conclusions on the impact of NIPPV in the hypoxemic subset of patients in our study because of small numbers. Systematic review, however, has suggested that the benefit of NIPPV extended to the hypoxemic respiratory failure patient, albeit with only modest benefits in clinical endpoints. [5] NIPPV has however been demonstrated in RCTs and meta-analyses to be beneficial in patients presenting with cardiogenic pulmonary edema. [4] It is interesting to note that 6 patients in our cohort had coexistent obesity that may have contributed to the respiratory failure. All these patients did well on NIPPV. Previous studies have reported improvements in clinical and biochemical endpoints in patients with obesity hypoventilation syndrome (OHS). [12],[13] Although we were unable to further evaluate our patients to document the coexistence of OHS, this area warrants further study. In the current study, the clinical improvement of patients on NIPPV was corroborated with improvements in the physiological variables. There was a significant improvement ( P < 0.001) in the average PaCO2 levels within an hour of application of NIPPV [Figure - 2A and B]. This change was also reflected in the pH, with improvements from 7.247 to 7.312 [Figure - 1A and B]. These physiological improvements are similar to that reported in literature in similar cohorts of patients. [1],[6] The severity of illness at presentation, as reflected by the APACHE II score, is postulated to influence response to NIPPV. Although two studies [14],[15] demonstrated a propensity for failure with NIPPV in patients with higher APACHE II scores, this observation has not been supported by other studies. [16],[17] The mean (SD) APACHE II score in the current study was 17.7 (4.5). Although the mean APACHE II scores were different between responders (17.2) as compared to nonresponders (20.2), this difference was not statistically significant ( P = 0.41). Other factors that have been previously shown to be associated with higher success rates include improvements in pH, PaCO 2 and respiratory rate after 1 h of initiation of NIPPV, along with an improvement in the level of consciousness. [9],[17] However, these could not be formally assessed in our study due to small numbers. The trend towards longer duration of hospitalization in patients who were treated successfully with NIPPV in the current study [Table - 3] may be a reflection of early deaths in those who failed NIPPV; however, this was not statistically significant ( P = 0.56). NIPPV aims to circumvent the complications of invasive mechanical ventilation like ventilator-associated pneumonias (VAP) and barotrauma while retaining the benefits of positive pressure ventilation. VAP rates are high in mechanically ventilated patients, with 8-28% of patients developing this problem. [18] Only 3 patients (7.5%) in our study developed a new patch on the X-ray associated with fever, tachypnea and leucocytosis, suggesting nosocomial pneumonia. [19] Although this incidence rate is much smaller compared with VAP rates from reported literature (above), it is similar to VAP rates in our institution (8%) from a recent study. [20] Despite the extensive descriptive nature of this study on a carefully selected group of patients treated in a medical ICU in a developing country, the lack of a control arm without the intervention (NIPPV) limits the impact of the study. Although a concurrent case control study would have given more credence to the study, we felt that withholding NIPPV would be inappropriate, given the evidence of benefit in other studies. A retrospective case control study was again not considered given the potential for bias in selection of controls. Determinants of success of NIPPV (like level of consciousness, functional status before ARF, comorbidities, BMI and hemodynamic state, etc.) were not evaluated as the study did not address this; and this is yet another limitation. However, it is interesting to note that the respiratory rate at admission was significantly higher in NIPPV nonresponders compared with NIPPV responders [Table - 3] and this could possibly be used to predict response to NIPPV. Admission respiratory rate [21] and fall in respiratory rate with NIPPV have been shown to be associated with success with NIPPV. [22] Notwithstanding these limitations, this study has demonstrated that NIPPV is not only a feasible ventilatory modality in developing countries but also a treatment that is associated with significant improvements in physiological and clinical outcomes. The application of NIPPV resulted in low rates of endotracheal intubation, fewer complications and was well tolerated in our cohort of patients. Although a cost-benefit analysis would have provided an impetus to NIPPV use in developing countries such as ours, lower initial cost of noninvasive ventilators (compared with standard ventilators), reduced duration of hospitalization and complication rates are likely to translate to favorable economic benefits. Further implications regarding the use of NIPPV need to be addressed in the context of a developing country such as ours. Newer modalities of treatment such as NIPPV require trained staff that can not only introduce and implement such therapies but also enable such treatments to translate to improvements in patient and clinical outcomes. We were fortunate to have faculty who obtained skills in NIPPV abroad and who subsequently trained the dedicated medical and nursing staff, as well as respiratory therapists, on the use of NIPPV and supervised patient care. Within a few months, NIPPV became an integral part of the respiratory support armamentarium of the unit. This was also achieved without additional staffing as the same technical and nursing staff looked after such patients. There was, however, additional cost of procuring dedicated bi-level ventilators. This may not be much of a problem now, given that modern ventilators could be used for both invasive and noninvasive ventilation. It would be interesting to assess, in future studies, if there is an impact of increased utilization of NIPPV on outcomes as this mode of treatment gains wider acceptance as an initial modality of treatment in our country for patients presenting with acute respiratory failure. References
Copyright 2007 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms07081f1.jpg] [ms07081f2.jpg] [ms07081t5.jpg] [ms07081t4.jpg] [ms07081t3.jpg] [ms07081t1.jpg] [ms07081t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}