 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
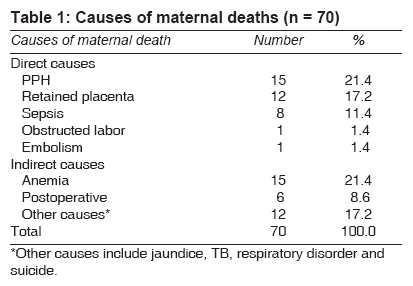
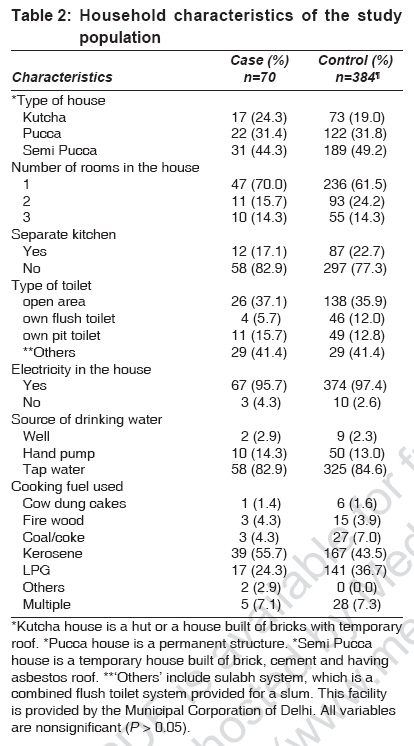
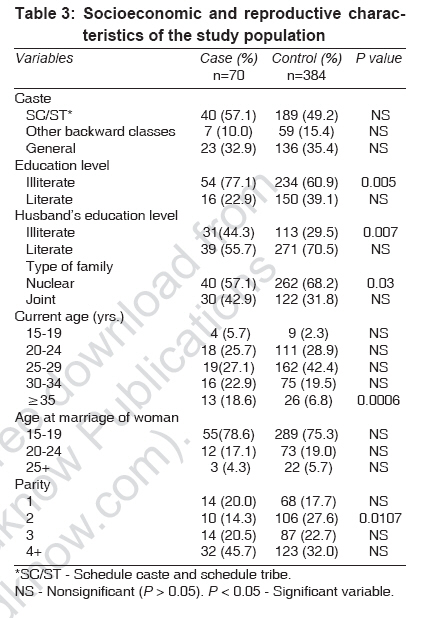
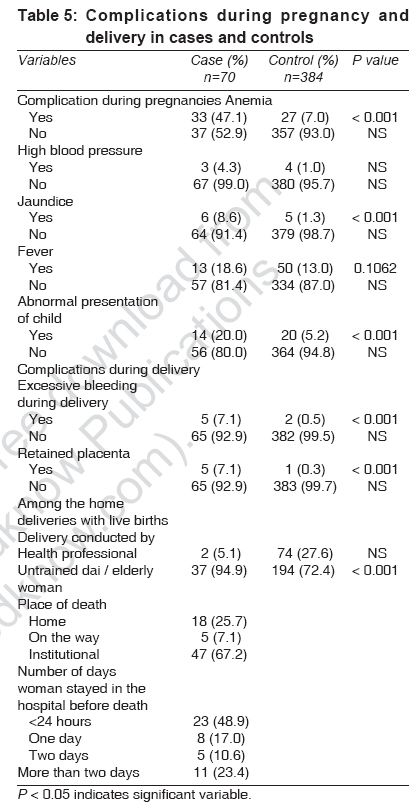
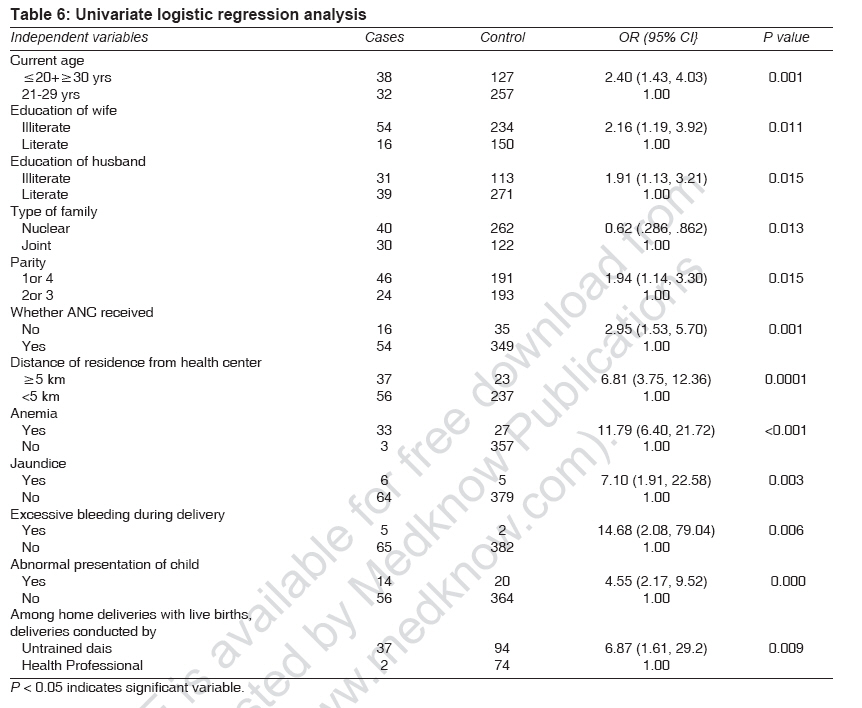
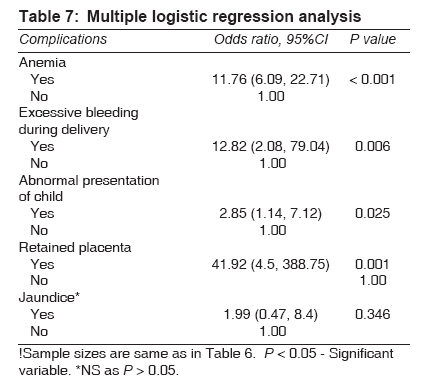
Indian Journal of Medical Sciences, Vol. 61, No. 9, September, 2007, pp. 517-526 Original Contributions Risk factors for maternal mortality in Delhi slums: A community-based case-control study Aggarwal, Abha; Pandey, Arvind; Bhattacharya, B.N. National Institute of Medical Statistics, Indian Council of Medical Research, New Delhi Code Number: ms07084 Abstract Background : In order to develop, implement and evaluate policy for reducing maternal mortality, it is essential to study the risk factors associated with maternal deaths.Aims : The study aims to determine the epidemiological risk factors and its related causes associated with maternal deaths in Delhi slums. Materials and Methods : A community-based case-control study was designed, wherein snowball-sampling method was used to identify the maternal deaths (cases) in the community, and circular systematic random sampling procedure was used to select the controls from the same area where a maternal death was found. Statistical Analysis : Data on 70 cases and 384 controls that had live births as the outcome of the pregnancy were analyzed. Logistic regression was applied to identify the risk factors. Results: In the study population, most of the deliveries were conducted at home by untrained 'dais.' Cases were mostly illiterate, young, having high parity and no antenatal care taken during pregnancy (P < 0.05) as compared to controls. The distance of health facility from residence was also found to be a significant risk factor for maternal death (P < 0.05). Complications during pregnancy, like jaundice, excessive bleeding and anemia, were also found to be significant. The major causes of maternal death were found to be hemorrhage after delivery, retained placenta and anemia. Conclusions : The study findings suggest that women should be educated about the importance of antenatal registration and regular checkups. Untrained 'dais' should be trained to recognize the obstetric complications at an early stage and refer high-risk cases for adequate management. These preventive measures could help in reducing maternal mortality at the community level. Keywords: Case control study, maternal mortality, risk factors, snowball sampling Pregnancy complications and childbirth-related complications are the major causes of death among women in their reproductive ages. Around 529,000 women die each year from maternal causes; and for every woman who dies, approximately 20 more suffer from injuries, infections and disabilities during pregnancy or childbirth. This means, at least 10 million women incur this type of damage every year. [1] Although various safe motherhood initiatives have been taken, yet decline in maternal mortality ratio (MMR: defined as maternal deaths per 100,000 live births) in India is far from the desired level of 100 by 2012 set by the National Rural Health Mission (NRHM) and 109 by 2015 as per millennium development goals (MDG). The level of MMR in India has declined from over 750 in the sixties to about 400 in the nineties. [2],[3] Recent round of sample registration system has estimated the level of MMR in India to be about 300 in 2001-03. However, the level of MMR is above 400 in some of the states [4],[5] encompassing over 40% of India′s population. This invites the attention of researchers to examine the causes and epidemiological factors associated with maternal deaths. In the past, there have been some studies which have identified adolescent pregnancy, short interval between pregnancies, multi-parity and distance from referral hospitals as the bio-behavioral risk factors. [6],[7],[8],[9] However, these studies are mostly descriptive and conducted in hospitals. Since majority of the deliveries in India are conducted by traditional birth attendants (TBAs), hospital-based estimates may not reveal the real picture. In the populations where obstetric care is poor and the lifetime risk of maternal death is much higher, it is essential to study the specific causes of such maternal deaths. In addition, abortion-related maternal deaths are often not accounted by these studies. Such issues are significantly prevalent in slums and underserved populations. In this context, a community-based case-control study was designed in Delhi slums FNx01 to determine the epidemiological risk factors of maternal deaths and their related causes. Further, the relative importance of each of these factors has been estimated by determining its relative risk through odds ratio using logistic regression analysis. Materials and Methods This study was a community-based case-control study, wherein a ′case′ was defined as a woman who was pregnant and whose pregnancy′s outcome was a live birth but the woman died within 42 days of delivery. A control was defined as a woman who was pregnant and whose pregnancy′s outcome was a live birth and the woman was surviving at the time of survey. Out of a total of 929 designated slums in Delhi, the study was conducted amongst 328 slums where the eighth India Population Project (IPP-VIII) was implemented. The population of these slums was approximately 1.25 million. This population was catered by 21 health centers, 6 maternity homes and 105 heath posts. A maternity home covered a population of 2 million; and for every 50,000 population, there was one health center and for every 10,000 population one health post was created. [10] These health centers were visited to capture the information regarding maternal deaths. The information of maternal deaths that occurred during the reference period, viz., April 2000-March 2003, was collected from the registers maintained at health centers. In addition to this, snowball-sampling method was used to capture all the maternal deaths in the community. [5] Snowball sampling for the selection of cases Data collection Study population Circular systematic random sampling for selection of controls Statistical analysis Results As mentioned, the results are presented for 70 cases and 393 controls. It was found that major causes for maternal deaths were anemia and hemorrhage after delivery (PPH) (21.4% each), retained placenta (17.2%) and sepsis (11.4%). The analysis revealed that 43 (61.4%) maternal deaths occurred due to direct causes and 27 (38.6%) due to indirect causes, which included 15 maternal deaths (55.5%) due to anemia. Other indirect causes included jaundice, TB, respiratory disorder and suicide. About 9% of the cases developed postoperative complications, and about 1% had obstructed labor [Table - 1]. No significant difference was found in household characteristics, viz., type of house, number of rooms, type of toilets, electricity, etc., in cases and controls, indicating that they were similar [Table - 2]. About 77% of cases were illiterate as compared to 61% in controls ( P < 0.001). The age of 79% of cases and 75% of controls at marriage was between 15 and 19 years ( P > 0.05). More than 65% of controls were living in nuclear families; while in cases, it was about 57% ( P = 0.03). Against 28% cases, 14% controls had parity 2 ( P = 0.017) [Table - 3]. A significant proportion, 23% of cases, did not register for ANC as compared to 9% in controls ( P < 0.001). Further, more than 60% of maternal deaths occurred in those households who lived> 5 km away from a health facility ( P < 0.001). To reach the health facility, the mode of transport used by the women included walking, manual rickshaw, auto rickshaw and taxi/van. Significant differences were found between cases and controls in using the manual rickshaw / auto rickshaw as the means of transport ( P < 0.001). Home delivery was observed in 55.7% of cases and 69.8% of controls, while institutional delivery took place in 44.3% of cases and 30.2% of controls ( P = 0.02) [Table - 4]. Complications encountered during pregnancy varied and included anemia, high blood pressure, fever, jaundice, abnormal presentation of child, excessive bleeding during delivery, retained placenta ( P < 0.001). However, no significant difference was found between cases and controls in regard to high blood pressure and fever ( P > 0.05). Among home deliveries, in cases 94.9% of the deliveries were conducted by untrained dais /elderly ladies; while in controls, 72.4% were conducted by untrained dais ( P < 0.001). The study shows that 67.2% of maternal deaths occurred at a health institution, 25.7% maternal deaths occurred at home and 7.1% died on the way to a health facility. Of the 67.2% institutional deaths, about 49% maternal deaths occurred within 24 h (day 0) of delivery, 17% on day one, 10.6% on day two and 23.4% maternal deaths occurred after two days from the day of delivery [Table - 5]. Univariate logistic regression analysis shows that the risk of dying of a woman in the categories of age ≤20 years and> 30 years was more (OR = 2.40; CI = 1.43-4.03; P = 0.001). The risk for maternal death was higher among illiterate women (OR = 2.16; CI = 1.19-3.92; P = 0.011) than among literate women. Similarly, the risk was twice in case of women who had either parity 1 or more than 4 as compared to women having parity 2 or 3 (OR = 1.94; CI = 1.14-3.30; P = 0.001). Further, the risk of dying for a woman due to no ANC registration was about three times more as compared to those who had registered for ANC care [Table - 6]. The risk of maternal death was higher where the distance of the health facility from the residence was> 5 km as compared to a distance < 5 km (OR = 6.81; CI = 3.75-12.36; P = 0.0001). Jaundice, excessive bleeding during delivery and abnormal presentation of child were also found to be the significant risk factors of maternal deaths. The risk for maternal death was seven times more if a delivery was conducted by an untrained dai at home as compared to those conducted by health professionals (OR = 6.87; CI = 1.61-29.2; P = 0.009) [Table - 6]. Multivariate logistic regression model was used to see the joint effect of complications like anemia, jaundice, excessive bleeding during delivery, abnormal presentation of child and retained placenta on maternal deaths. The model was found to be a best fit model (c2(1) = 0.446; P = 0.406), indicating that the assumed hypothesis is accepted. Results show that the risk of maternal death was more among anemic women (OR = 11.76; CI = 6.09-22.71; P < 0.001). Similar risk was found in case of excessive bleeding during delivery as compared to women with normal bleeding. The risk of maternal mortality associated with retained placenta in the presence of other complications was (OR = 41.92; CI = 4.5-388.75; P = 0.001). Abnormal presentation of child was also found to be a risk factor (OR = 2.85; CI = 1.14-7.12; P = 0.025). It indicates that the risk for maternal death was about three times more in women with abnormal presentation of child as compared to normal presentation. Jaundice was found to be a confounding complication in multiple logistic regression ( P > 0.05) [Table - 7]. Discussion This study was conducted in the urban slums in Delhi to investigate the epidemiological risk factors associated with maternal mortality using a cost-effective snowball-sampling technique. [5],[11] The major direct causes of maternal death in the study were found to be PPH, followed by retained placenta and sepsis. The data, particularly those of PPH and sepsis, are comparable to those reported elsewhere. [5],[12],[13] However, as per the report of the sample registration system (SRS), hemorrhage has been reported to be 38%, which is much higher than our estimate. Since SRS included all maternal deaths irrespective of the outcome of pregnancy, i.e., including abortions and stillbirths, against ours, which has considered only those maternal deaths where the outcome of pregnancy was only live birth; hence the former estimates are likely to be higher than ours. The estimates of sepsis were, however, comparable to our estimates. [4] Contrary to reported literature that hypertensive disorders are one of the causes of maternal deaths, [4] our study did not find any such case, probably because the outcome of pregnancy included only live births. Also, our study was carried out in the slums of Delhi, where a large section of the pregnant women do not utilize the facility of ANC; and therefore, no case of hypertensive disorder was reported to have been included in the study. Further, the cause of death was elicited by the gynecologist through verbal autopsy after the death of the woman - based on the information collected from family members, who may not have been aware of any hypertensive disease. The proportion of maternal deaths due to retained placenta in the present study was found to be marginally higher than those reported elsewhere. [13] In this context, it may be mentioned that as most of the deliveries were conducted at home, by untrained dais, they were unable to manage the cases that were even a little bit complicated. Retained placenta is potentially life threatening not only because of retention per se but also because of associated hemorrhage and infection, as well as complications related to its removal. These risks are increased in women in poor social circumstances due to preexisting malnutrition, anemia and unsupervised home deliveries. [14] Among the indirect causes, anemia was found to be the major cause of maternal death in the present study. Our findings are consistent with those of other researchers who have reported that direct causes together with anemia are responsible for more than 65% of all maternal deaths in developing countries. [4] Anemia remains a major problem among the women folk in India, and launch of the recent initiative of ′Twelve by Twelve (12 by 12),′ if successful, would go a long way in not only reducing the maternal mortality but also maternal morbidity. [15] Since the entire study population was from urban slums, wherein both cases and controls belonged to the same socioeconomic bracket with similar housing, water and toilet facilities, socioeconomic characteristics do not show statistically significant differences between cases and controls. Jaundice during pregnancy appears to be an important risk factor, which might have occurred due to poor sanitary conditions in and around the house. The study found that more maternal deaths occurred in younger women with high parity, living in joint families and with no ANC registration. The reason for not registering may be due to longer distance from the residence. Further, in joint families, pregnant women are more likely to be sidelined. It was found that among the home deliveries (39 cases), about 95% of the deliveries were conducted by untrained dais. Untrained dais are commonly sought after for conducting deliveries in rural and urban slum populations. Training them about safe delivery and immediate basic care of newborn infants and instructing them to refer to the nearest essential obstetric care unit if any danger signs become obvious may prove to be an important, cost-effective strategy to reduce maternal and neonatal mortality in communities. They can also contribute in terms of health education and encouraging breastfeeding. Investing in such training should be considered by policy makers and donor agencies. [16] In our study, a high proportion of maternal deaths occurred in hospitals. A possible reason for such a paradoxical finding is that probably the deliveries were conducted at home by untrained dais and were rushed to a hospital at the last minute when they became too complicated for untrained dais to handle, and hence a greater number of women died at a hospital. This is also evident from the fact that most of the admitted women died within 24 h of admission (48.9%). Conclusion Despite the many MCH programs in vogue, majority of cases had not even registered for ANC in the slum population and most of the deliveries were conducted at home by untrained dais. Preventive measures which could help to reduce maternal mortality include (1) mass education about the importance of antenatal registration and regular checkups and (2) more focus on training of dais. (3) Further, since the present study was conducted in the slums of Delhi, where institutional facilities and transport are more easily available than in the rural areas, women should be encouraged to go for institutional deliveries to reduce maternal mortality at the community level.Acknowledgements The authors are thankful to the Department of Family Welfare (Statistics Division), Ministry of Health and Family Welfare, GOI, for providing funds and entrusting this research study to National Institute of Medical Statistics. Thanks are also due to Dr. Mouha Maulik, Scientist, who helped in revising the manuscript. Mr. Jitendra Yadav and Mr. Ganesh Prasad Jenna are also duly thanked for conducting the field work.References
Copyright 2007 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms07084t1.jpg] [ms07084t6.jpg] [ms07084t5.jpg] [ms07084t2.jpg] [ms07084t7.jpg] [ms07084t4.jpg] [ms07084t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}