 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
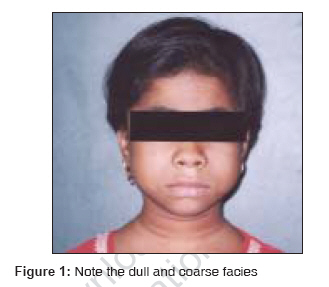
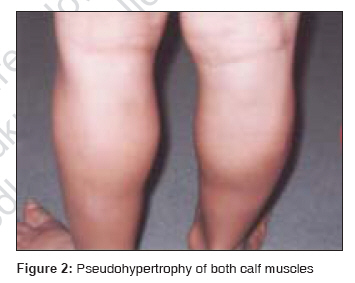
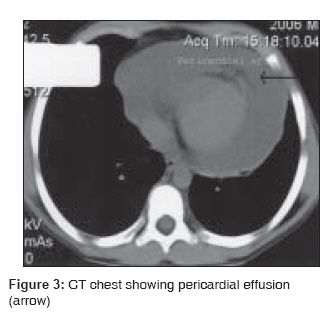
Indian Journal of Medical Sciences, Vol. 61, No. 9, September, 2007, pp. 527-530 Case Report Kocher-debre-semelaigne syndrome with pericardial effusion Dharaskar, Praveen; Tullu, MilindS; Lahiri, Keya R.; Kondekar, Santosh; Vaswani, Rajwanti K. Department of Pediatrics, Seth G.S. Medical College and K.E.M. Hospital, Parel, Mumbai Code Number: ms07085 Abstract We report a 10-year-old female child with hypothyroidism and limb muscle pseudohypertrophy (i.e., Kocher-Debre-Semelaigne syndrome) with pericardial effusion. The child presented with generalized swelling, breathlessness and difficulty in walking and in getting up from sitting position (of chronic duration). She had bradycardia, dull facies, marked hypertrophy of both calf muscles and nonpitting edema of legs. Pericardial effusion was detected clinically and confirmed on investigations. Muscle pseudohypertrophy was a striking feature, and hypothyroidism was confirmed on thyroid studies. The response to thyroxine replacement was excellent, with resolution of the pericardial effusion and clinical improvement. The unusual presence of pericardial effusion in Kocher-Debre-Semelaigne syndrome is discussed in the report. Keywords: Hypothyroidism, muscle, pericardial effusion, pseudohypertrophy, thyroxine Introduction Kocher-Debre-Semelaigne syndrome (also labeled as Cretinism-muscular hypertrophy, hypothyroid myopathy, hypothyroidism-large muscle syndrome, hypothyreotic muscular hypertrophy in children, myopathy-myxedema syndrome, myxedema-muscular hypertrophy syndrome, etc.) is a rare disorder causing pseudohypertrophy of muscles due to longstanding hypothyroidism. [1],[2] Pericardial effusion is known in hypothyroidism but has not been reported with Kocher-Debre-Semelaigne syndrome. Case Report A 10-year-old female child (resident of the state of Uttar Pradesh, India) presented with swelling all over the body and breathlessness since the last 2 years and difficulty in walking and in getting up from sitting position since 5 months. There was no history of palpitations, arthritis, oliguria or similar disorder in any family member. On examination she had a pulse rate of 76/min, respiratory rate of 24/min, blood pressure of 90/60 mmHg (low) and Tanner′s stage-I. Her height was 116 cm (expected 136 cm) and weight was 20 kg (expected 32 kg). The child had dull coarse facies [Figure - 1]; hypertrophy of muscles of all the extremities, especially the calf muscles [Figure - 2]; nonpitting edema of legs; and absence of goiter. On cardiovascular system examination, the apex beat was in the left 5 th intercostal space in the midclavicular line, the left heart border was in mid-axillary line (not coinciding with the cardiac apex), heart sounds were muffled and there was absence of any murmur. On central nervous system examination, the child had normal sensorium, the tone was normal with proximal muscle weakness (muscle power being 4/5, distal muscle power being normal), deep tendon reflexes were diminished, sensory system was normal, the plantar responses were flexor and rest of the systemic examination was normal. In presence of features of hypothyroidism, the pseudohypertrophy of muscles suggested a diagnosis of Kocher-Debre-Semelaigne syndrome (with pericardial effusion). Investigations revealed hemoglobin of 9.5 g% and leukocyte count of 7200 per mm 3 (polymorphs 70%, lymphocytes 30%). The CT scan chest [Figure - 3] and 2-D echocardiography were suggestive of pericardial effusion, the liver (normal total serum protein level of 6.7 g%) and renal function tests were normal and bone age was 8 years (delayed). Thyroid function tests showed total T3 < 40 ng/dl (normal 70-200 ng/dl), total T4 < 1 microg /dl (normal 5.5-13.5 microg/dl), TSH> 75 microIU/ml (normal 0.2-5.0 microIU/ml), which confirmed the diagnosis of hypothyroidism. USG showed normal thyroid gland, and the technetium scan showed normally positioned thyroid with poor uptake. Anti-microsomal antibodies were absent. Within 2 months of treatment with L - thyroxine (50 µg per day), the patient′s edema in the feet, pericardial effusion and muscular pseudohypertrophy decreased. The patient did not follow up for repeat thyroid hormone level estimation. Discussion Thyroid hormone deficiency, a cause of 5% cases of acquired myopathies, [3] is a treatable disorder. The association of hypothyroidism and muscle pseudohypertrophy is called as Kocher-Debre-Semelaigne syndrome. Usual age of presentation is between 18 months and 10 years, [1],[2],[3],[4],[5] but the reports of the condition being diagnosed in earlier age and neonatal age are also available. [1] The patients present with the clinical features of hypothyroidism along with muscle pseudohypertrophy. [1],[2] The pseudohypertrophy involves muscles of extremities, limb girdle, trunk, hands and feet but it is more prominent in muscles of limbs; hence the athletic or herculean look. [1],[2],[3],[4],[5],[6] The pathogenesis of the pseudohypertrophy is not still completely understood. It has been found to be associated with various forms of hypothyroidism, like absence of thyroid gland, defective synthesis of thyroid hormone or autoimmune causes of hypothyroidism. [2] The pseudohypertrophy is thought to be a result of the effect of longstanding hypothyroidism. [1] Ignorance of the patient and non-availability of medical care in remote villages may be the reason for the hypothyroidism to be missed in the present case. The patient actually sought medical attention on developing the symptoms of pericardial effusion. Our patient had weight which was relatively good for her height, and she did not have any features of malnutrition. There was absence of severe weight gain as may occur in patients with hypothyroidism. The diagnosis depends on the presence of clinical features and myopathic changes. The cause of hypothyroidism in our patient could be autoimmune thyroiditis probably due to TSHR-blocking antibodies (though we were not able to prove the same). CPK and SGOT enzyme levels are elevated, but the histopathological picture is not characteristic of the disease. [2],[3],[5],[6] Treatment with thyroid supplements has been shown to cause reversal of pseudohypertrophy and clinical symptoms. [2],[3],[4],[5] Kabadi et al. found that the incidence of pericardial effusion in hypothyroidism was only 6% (2 out of 30 cases). [7] The occurrence of pericardial effusion in hypothyroidism appeared to be dependent on the severity of the disease. Pericardial effusion may be a frequent manifestation in myxedema (30-80%), an advanced severe stage but is a rare association of hypothyroidism in an early mild stage. [7] Hypothyroidism is associated with increased capillary permeability and impaired lymphatic drainage with subsequent leakage of protein into the interstitial space, resulting in pericardial effusion, a common clinical finding in overt hypothyroidism. [7],[8] The presentation and clinical course of pericardial effusion in hypothyroidism are extremely variable. Pericardial effusion, a rare major presenting manifestation in hypothyroidism, is occasionally complicated by pericardial tamponade. [8] The rarity of cardiac tamponade in patients with pericardial effusion is attributed to the slow accumulation of fluid and the remarkable distensibility of the pericardium. [8] The effusions disappear after treatment with thyroxine. [7],[8],[9] The pericardial effusion is not a unique part of the syndrome but is probably due to longstanding or severe hypothyroidism. [10] Pericardial effusion has been documented in four infants with Down syndrome suffering from congenital hypothyroidism. [9] In addition to pericardial effusion, subtle evidence of alteration of myocardial function (which reverses on treatment) may also be seen in children with primary hypothyroidism. [10] An extensive literature search did not reveal report of pericardial effusion and Kocher-Debre-Semelaigne syndrome together (though pericardial effusion has been reported in patients with hypothyroidism), hence this report. Acknowledgments The authors thank Dr. N. A. Kshirsagar, Director (Medical Education and Health), Municipal Corporation of Greater Mumbai; and Dean, Seth G. S. Medical College and KEM Hospital, Mumbai, for granting permission to publish this manuscript.References
Copyright 2007 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms07085f1.jpg] [ms07085f3.jpg] [ms07085f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}