 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
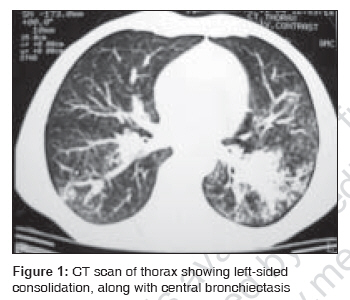
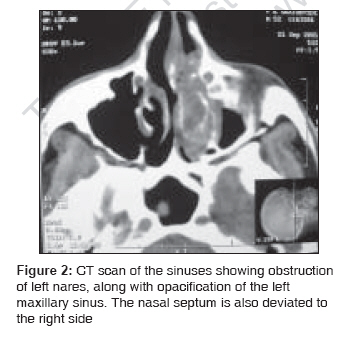
Indian Journal of Medical Sciences, Vol. 61, No. 9, September, 2007, pp. 532-534 Letter To Editor Concomitant allergic bronchopulmonary aspergillosis and allergic fungal sinusitis Prasad, R.; Garg, R.; Sanjay, Ruchi Dua Department of Pulmonary Medicine, King George's Medical University, Lucknow Code Number: ms07087 Sir, The presence of concomitant allergic fungal sinusitis (AFS) and allergic bronchopulmonary aspergillosis (ABPA) in the same patient represents analogous process of fungal hypersensitivity in the upper and lower airway, which is also known as sinobronchial allergic mycosis (SAM) syndrome, and is rarely reported. [1],[2] A 52-year-old nonsmoking married male, bank clerk by occupation, presented with complaints of episodic breathlessness and cough with minimal expectoration for the last 10 years and recurrent hemoptysis for the previous 6 years. There was no family history suggestive of allergic diseases. Bilateral diffuse rhonchi were audible on chest auscultation. On investigation, total leukocyte count was 10,800/mm 3 , with eosinophils being 12% (absolute eosinophil count 1,296/mm 3 ) on differential count. Spirometry showed features of mild obstruction (FEV1 67%, FEV1/FVC ratio 60) with significant bronchodilator reversibility (310 ml [% change 15]). Skin-prick tests with Aspergillus fumigatus antigen showed a positive reaction for type I hypersensitivity. Total Immunoglobulin E was 5,652 IU/ml (reference range 0-100 IU/ml). Specific Immunoglobulin G and Immunoglobulin E against A. fumigatus by ELISA was raised, 66.30 and 159.90 IU respectively (< 0.35 kUA/L normal range). Computed tomography (CT) of thorax revealed left-sided consolidation, along with central bronchiectasis [Figure - 1]. On further evaluation, the patient also gave history of recurrent nasal discharge for 25 years, which persisted despite long-term medical treatment. Nasal examination demonstrated an edematous nasal mucosa, nasal polyp and thick mucus. CT scan of the sinuses revealed hyperdense lesion in the left ethmoid and maxillary sinus without any bony erosion, along with deviated nasal septum on right side [Figure - 2]. Functional endoscopic sinus surgery was performed with a left-sided polypectomy and maxillary antrostomy. Microscopic examination of material from maxillary sinus showed allergic mucin with eosinophils, and culture grew Aspergillus species . Thus he was diagnosed as a case of ABPA with AFS and was started on a single daily dose of 40 mg prednisolone (0.5 mg/kg), along with topical nasal steroid by inhalation, montelukast sodium (10 mg/day) and inhaled salmeterol with fluticasone dipropionate 500 mcg two times per day from a metered dose inhaler. At the present time, the patient continues to do well. All asthmatics with a positive skin-prick test to aspergillus antigens must be evaluated for ABPA. [3] AFS is a noninvasive form of fungal sinusitis that is seen in highly atopic individuals with Aspergillus -specific IgE, intractable sinusitis and nasal polyposis. [4] While the diagnosis of AFS is primarily based on histopathology, roentgenology is essential for the diagnosis. Haziness of one or more paranasal sinuses is almost always seen on plain roentgenograms. However, CT offers more reliable information with characteristic features that include heterogeneous densities and serpiginous areas of increased attenuation. [5] Since asthma and sinusitis are often seen by two different specialties, the occurrence of AFS in ABPA and ABPA in AFS may easily be overlooked. Therefore, a high index of suspicion is required for the diagnosis of AFS, and a patient with history of asthma and/or rhinitis should be investigated for ABPA and/or AFS. References
Copyright 2007 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms07087f1.jpg] [ms07087f2.jpg] |
| |||||||||

{kind=link}
{kind=link}