 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 61, No. 9, September, 2007, pp. 535-544 Practitioners section How the findings of national family health survey-3 can act as a trigger for improving the status of anemic mothers and undernourished children in India: A review Lahariya, Chandrakant; Khandekar, Jyoti Department of Community Medicine, Gajara Raja Medical College, Gwalior; Department of Community Medicine, Lady Hardinge Medical College, New Delhi Code Number: ms07088 Abstract The national family health survey-3 (NFHS-3) reports of declining fertility rate while increasing prevalence of anemia in women and children, since NFHS-2 in 1998-99. The proportion of anemic, stunted and wasted children has also increased since the previous two rounds. NFHS trends show that the status of mother's and child's health indicators is continuing to deteriorate in spite of the many government-run targeted programs, e.g., integrated child development scheme (ICDS), Midday meal program. The only good sign in the findings is the favorable trend in fertility indicators and infant mortality rate. A review of the findings of NFHS surveys, the current government policies and programs targeted upon the improving of health status of women and children in India and of the published scientific literature was conducted. The aim of the review was to understand the health situation of women and children in India and to suggest measures to bring about positive changes in the health status of this population. The analysis suggests that the findings of these successive surveys are not being utilized for the necessary corrective measures. The authors argue that although the NFHS is a useful exercise, in the wake of decentralized planning, the country needs more detailed data focusing on the districts. Synchronization of the ICDS and national rural health mission (NRHM), along with entrusting the responsibility of conducting NFHS to the planning commission, is the other possible solution to tackle the problems of rising anemia and malnutrition in the country. Keywords: Anemia, immunization, India, national family health survey, nutrition The last few years have generated a demand for strong information system for proper planning in the field of health. The most essential information, to start with, is the baseline data on health indicators, for carrying out monitoring and evaluation in various programs and activities. For a long time after independence, evaluation had only limited focus and no separate resources were made available for collection of information on the health status of the population. The need for countrywide health information was felt strongly in the early nineties, and the first national family health survey (NFHS) was conducted in 1992-93. [1] The NFHS, is one of the largest household surveys conducted in India. The NFHS aims to help the planners and policy makers in the process of informed decision making, besides keeping a track of the health trends in the country. The first survey (NFHS-1) was conducted in 1992-93, followed by second survey (NFHS-2) in 1998-99. [2] NFHS-3 is the latest in this series. The preliminary results from NFHS-3 show decline in fertility rate and infant mortality rate (IMR) but rising prevalence of anemia in women and children and almost static and high prevalence of malnutrition in children aged less than 3 years, since NFHS-2. The indicators of health-seeking behavior also show negative trends. This paper is based upon the secondary analysis of NFHS-3 data released by International Institute of Population Sciences (IIPS), India, and analyzes the findings of this NFHS-3 in the perspective of the health scenario in India. This review was conducted with the aims of understanding the health situation of the mothers and children in India and suggesting measures to bring about positive changes in their health status. How This Review was Conducted Keeping in mind the aims of this review, all the published reports of NFHS-1 and NFHS-2 were studied, along with the study of the preliminary reports of the current round of the NFHS. The main focus was on the trends of the health indicators since the NFHS-1. The critical commentaries, scientific publications and other reports on NFHS were also collected and studied. PubMed search engine, libraries and internet resources were used for this data collection. A detailed information search on the various government policies and programs targeted upon improving the health status of women and children was carried out. This paper is based upon the trend analysis of NFHS findings, in the background of various health programs being run in the country.Methodology of NFHS -3 The planning of NFHS-3 had started in February 2005 and the field work was done from December 2005 to August 2006, covering all 28 states and Delhi. It was conducted under the guidance of the Ministry of Health and Family Welfare (MOHFW), with International Institute of Population Sciences, Mumbai, as nodal agency. The ORC Macro, USA, provides technical assistance, with funding from five international (USAID, DFID, UNFPA, UNICEF, Bill and Melinda Gates Foundation) and two national agencies (NARI and NACO), besides partial funding by the Government of India. The objectives of the NFHS-3 are twofold - firstly, to provide essential data on health and family welfare needed by Government of India and other agencies for policy and program purposes; and secondly, to help in measuring the trends in the health and family welfare issues. The interview schedules were used for data collection by trained investigators. The interviews were conducted with eligible respondents using a Household Questionnaire, a Woman′s Questionnaire (for women aged 15-49) and a Man′s Questionnaire (for men aged 15-54). Total 18 research organizations conducted interviews with more than 230,000 women (age 15-49 years) and men (age 15-54 years) throughout India. NFHS-3 also tested more than 100,000 women and men for HIV and more than 200,000 adults and young children for anemia. [1] The information and activities carried out can be clubbed as follows:
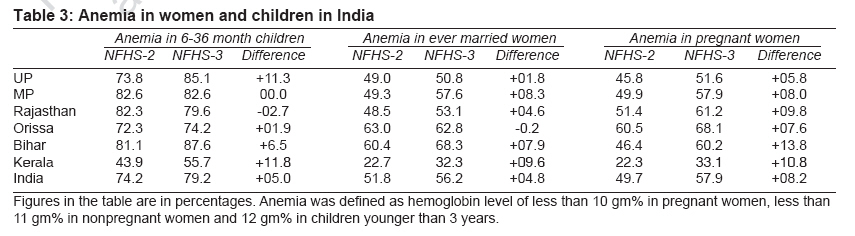
The NFHS-3 has collected information on several new and emerging issues (which were not covered in the previous round), including perinatal mortality, male involvement in family welfare, adolescent reproductive health, high-risk sexual behavior, family life, education, safe injections, tuberculosis and malaria. It also focused upon family welfare and health conditions among slum dwellers in eight large cities. For the first time ever, blood samples have been collected to know the HIV prevalence at the national level and in the five high-prevalence states. [1] The methodology received ethical approval from the MOHFW and independent ethical approval committee of independent experts. [1] The blood sample collection for both HIV testing and hemoglobin estimation was standardized and collection was done after informed consent of the subjects as approved by the ethical committee. It was decided to keep the HIV testing as ′unlinked and anonymous′ and the results of such testing were used for survey purpose only. The details of the procedure are available on IIPS website. [1] The outputs of NFHS-3 have been planned in the form of state and national fact sheets, national report in two volumes, state reports, specialized subject reports, key findings report and wall charts. The states and India fact sheets are the first in the series of the findings to be released. These fact sheets provide information on fertility, family planning, age at marriage and first child birth; and maternal health indicators like three ANC visits, institutional deliveries, childhood immunization, health-seeking behavior, nutritional status and anemia, besides knowledge of adult population on HIV/AIDS and women empowerment. [3] The details of methodology can be found on the website of IIPS. [1] This paper analyses the information available from the NFHS-3. Special attention has been given to the five empowered action group (EAG) states (Uttar Pradesh, Madhya Pradesh, Bihar, Rajasthan and Orissa). The indicators of Kerala state and India have been provided for comparison. The EAG states have been identified for this review as they are known for poor performance on majority of the health indicators and constitute more than 40% of the total population of the country. No health goal is achievable unless the performance of these states is improved. Even the planning commission of India recognizes their special needs for planning and policy-making purpose. [4] Results of NFHS-3 During the past 13 years, since the first NFHS, there has been continuous decline in fertility in India. Some states have reached the replacement level of fertility, viz., Kerala, Punjab and Maharashtra; while the total fertility rate (TFR) in states like UP and MP is very high - at 3.82 and 3.12 respectively. Bihar has been found to show a trend of increasing fertility too [Table - 1]. The decline in TFR is noticeable across the country although the progress is slow in the EAG states. The urban areas in majority of the states have either reached TFR of replacement level or are very close to doing so. The wide rural-urban difference is still continuing - viz., the TFR in urban Orissa has gone to a level below 2, while TFR in rural areas of UP is well above 4. [2],[3],[5] Maternal health Child health There is a fall in the proportion of the parents going to the health facility in cases of illness of their child since NFHS-2. The proportion of children who received ORS for the last episode of diarrhea has decreased in most of the states and ranges from 12-41%. Nutrition and anemia The overall proportion of undernourished children has increased in the country since NFHS-2; and in the states of MP, UP and Bihar, almost 85% of children were found to be anemic. As many as 74% of this population group are anemic in India, with prevalence of anemia in UP as high as 85.1%. What is more worrisome is the increasing prevalence of anemia since NFHS-2. This proportion is higher than both the previous rounds of NFHS. The total prevalence of wasting among children has also increased from 15% in NFHS-2 to 17% in this round. More than half to two-thirds of women, whether pregnant or not, are anemic. This prevalence has risen since NFHS-2; and in some cases, since NFHS-1 also. Anemia is not restricted to women and children only. Adult men are also commonly affected with the problem of anemia, and up to two-thirds of men are anemic, with uniform distribution. [1] Discussion The NFHS-3 data can very well be taken as an alarming bell. Increasing anemia, malnutrition and decreasing utilization of health services must be the signs of concern for the planners. While the falling TFR and rising couple protection rate (CPR) are some signs of hope, the progress in EAG states is a bit slow but trends are favorable. The rural areas are still lagging far behind, and the planners need to think of targeted interventions in these states and areas, addressing issues like son preference, low rate of male sterilization, etc. Limited decision-making power to women is detrimental to fertility control as even a mother wants family planning, but she cannot decide for herself. The empowerment of women will be a health-improving measure. The NFHS-3 findings show an inverse relationship between fertility and the educational status of the mother. When making a comparison between the fertility of women with no education and those with 10 or more years of education, a difference of two children is noticeable in majority of the states. [3] Decreasing fertility may be attributable to increased CPR, increased age at marriage and increased age at the first child birth, as reported in NFHS-3. [3] Smaller contribution of male sterilization, which is also falling ever since NFHS-1, is another area of concern. [6] The data on the nutritional status of children aged less than 3 years does not give a good picture. The schemes like ICDS and midday meal are being praised at many a places. [15] There seems to be almost no excuse for almost half of the children under the age of 3 years being undernourished. What is more worrying is that this proportion has increased since NFHS-2. The absolute level of anemia has increased, and there are adverse trends in NFHS-3. Children (6-35 months) and pregnant women, the most vulnerable sections of our population, are suffering more and more in an era of economic growth of India. This high level of malnutrition increases the chances of getting infections and leading to high mortality levels, especially infant mortality and maternal mortality. Improved fertility indicators would be hollow if this same population continues to be anemic and malnourished. The family planning program has been rechristened and redesigned many a times, but the main focus still seems to be ′fertility control.′ Infants and children do not appear to get the desired attention, and the low rate of postpartum visits may be a dummy indicator. Immunization coverage in India has fallen, and the states which are most affected are EAG states. [16] Occasionally, researchers have attributed this to the repeated pulse polio activities also, but that cannot be a complete explanation. [17] The proportion of fully immunized children is less than half in majority of the states. Immunization activities in RCH program seem to be relegated as a secondary work. This component needs rethinking and restructuring after careful evaluation. It is not that everything is bad with NFHS. It has some features that need to be mentioned, e.g., timely release of data. The timeliness in disseminating the results of national surveys is essential for planners and policy makers. Lengthy time lags between data collection and tabulation invariably make the data obsolete. The same pace should be there for taking corrective measures based upon these findings. Detailed information on a number of health indicators is a distinct advantage of NFHS over other surveys conducted in the country, viz., census, sample registration system. [18] Secondly, the conducting of NFHSs by an independent agency, without any control of government, either in funding or in technical assistance, increases reliability and acceptability of the results. The NFHSs are laudable efforts only if the findings are used for corrective measures. The current trends in health indicators do not suggest that serious action is being taken to improve the health scenario or program in the country on the basis of NFHS findings. The whole exercise is futile if no corrective measures are taken. The NFHS findings need to be given more attention by both national and state governments for planning and resource allocations. Finally, planning of such a massive survey is a Herculean task, but even such a big survey does not provide district-wise data (because the sample size does not permit generalizing at the district level); this is one great weakness. India′s incredible diversity makes district data an absolute necessity to get at reality. At a time when decentralization has become a buzzword, state level data have limited value. The district level data may be useful for planning and also for monitoring and assessing the impact of numerous developmental programs at the local level. The Union Ministry of Health and Family Welfare had started such useful district level surveys, initially called reproductive and child health (RCH) surveys and now called district level household surveys (DLHS), in the year 2002. [19] The data generated by these surveys are far more useful than NFHS data, but these are hardly discussed and used. The state-level data are good and give a large picture of the states. What is equally required is the district-level health information so that necessary action may be taken at the right place. The DLHS should be done in the inter-NFHS period to make NFHS data more useful. These surveys can be a difficult and massive exercise. Initially, this exercise may be restricted to poorly performing states as per NFHS. Triggers from NFHS-3
Conclusions This review suggests that NFHS is a good exercise, which generates data to be utilized for planning, monitoring, evaluation and resource allocation to various programs in India. The findings of NFHS-3 point out that there has been almost no improvement in the health status of women and children in India for the last 15 years, and in some cases their condition has even deteriorated. The most probable reason is that the results of these successive surveys are not being utilized for the stated objective of taking corrective measures in the programs. The NFHS-3 should act as a trigger for a new beginning. The immediate focus of the country should be on improvement of health status of women and children; immunization strengthening; increased access to basic medicines like iron tablets, and ORS and health facilities for the poor people. At a time when one of the most ambitious programs on health, NRHM, is being rolled out, it is very pertinent that these findings are used for decision making. Besides, the DLHS should be made routine exercise during the inter-NFHS period. The idea of Planning Commission using the findings of NFHS-3 for resource allocation also needs immediate attention. These efforts should bring about some positive changes in the health status of this population; and who knows, we may achieve what have been elusive health goals for many years when India conducts the next round of NFHS, somewhere in 2012 or 2013. References
Copyright 2007 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms07088t3.jpg] [ms07088t2.jpg] [ms07088t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}