 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
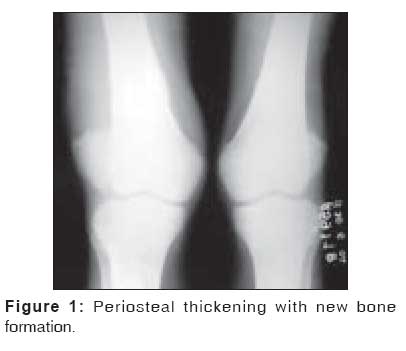
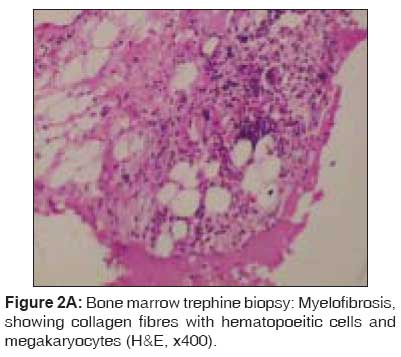
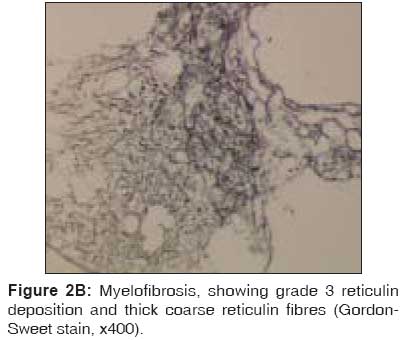
Indian Journal of Medical Sciences, Vol. 62, No. 2, February, 2008, pp. 65-68 Case Report Unusual associations of pachydermoperiostosis: A case report Kumar Uma, Bhatt SuryaPrakash, Misra Anoop Department of Medicine, All India Institute of Medical Sciences, Ansari Nagar, New Delhi Correspondence Address:Dr. Uma Kumar, Department of Medicine, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029, India. E-mail: umaakumar@yahoo.co.in Code Number: ms08011 Abstract Primary hypertrophic osteoarthropathy (HOA), or pachydermoperiostosis, is a rare benign disorder of unknown etiology. It is characterized by clubbing, periosteal reaction, and thickening of the skin. Disease usually progresses slowly, and natural arrest may occur. Reported herein is the case of a 28-year-old male patient with progressively increasing swelling of large joints of lower limbs with severe anemia. He was diagnosed as a case of pachydermoperiostosis with myelofibrosis, which is a rare association. The development of myelofibrosis makes primary HOA a disease with unfavorable outcome.Keywords: Empty sella syndrome, HOA, myelofibrosis, pachydermoperiostosis Introduction Primary HOA comprises about 3-5% of all cases of HOA. A positive family history is seen in about one-third of the cases, with an autosomal dominant mode with variable penetrance being the most common inheritance pattern. [1] It has a bimodal age distribution, with one peak in the first year of life and another at 15 years of age. Various rare associations like hypertrophic gastropathy, peptic ulcers, gynecomastia, acro-osteolysis of fingers and toes, Crohn's disease, and bone marrow failure due to myelofibrosis have been described. Only six cases of myelofibrosis in primary HOA have been described so far. [2],[3],[4],[5],[6] We describe a rare association of this usually benign condition with myelofibrosis and its possible association with primary empty sella syndrome. Case Report A 28-year-old man presented with an 8-year history of easy fatigability and progressive swelling of both ankles and knees. There was no history of arthralgia, backache, fever, oral ulcerations and photosensitivity, bleeding from any site, dyspnea, cough, and weight loss. He had significant family history, with two of his sisters suffering from the same ailment. On general physical examination, the patient was pale, with coarse facial features, sebaceous hyperplasia, and furrowing of forehead. He also had widened wrists and ankles, with grade four clubbing. Joint examination revealed nontender bilateral knee joint effusion. Systemic examination revealed 4-cm enlargement of the spleen, which was firm and nontender. Rest of the examination was unremarkable. Investigations revealed hemoglobin of 5.8 g/dL, with a corrected reticulocyte count of 1%. Peripheral smear examination revealed ovalocytes and teardrop cells. The total leukocyte count and platelet count were normal, with ESR of 70 mm in the first hour. Serum iron studies showed iron deficiency anemia. Coomb's tests (direct and indirect) were negative. Serum calcium, phosphate, alkaline phosphatase, and liver function tests were normal. Baseline investigations to rule out a secondary cause for clubbing revealed a normal chest x-ray and echocardiography. Stool analysis was negative for occult blood. Ultrasound abdomen showed splenomegaly. X-rays bilateral knee joint showed shaggy periosteal reaction of long bones bilaterally with distal soft tissue swelling [Figure - 1]. Synovial fluid analysis was not contributory. Bone marrow aspiration was dry, and examination of the biopsy revealed a hypoplastic marrow with grade 3 myelofibrosis [Figure - 2]A and B. Further investigations to rule out common differentials like pituitary growth hormone excess revealed an empty sella [Figure - 3]. Visual field charting did not show any field defects. Hence the patient was diagnosed as having primary pachydermoperiostosis with myelofibrosis and empty sella syndrome. Discussion The most common clinical features of primary HOA include clubbing (89%); periosteal new bone formation (97%); coarsening of skin, seborrhea (90%); acne, folliculitis, palmo-plantar hyperhydrosis (44-67%); partial ptosis and cutis verticis gyrata (24%). Common clinical presentations include progressive widening of distal part of long bones, bulbous deformities of fingers and toes, synovial effusions (41%); arthritis (20-40%); and paresthesias. The skeletal involvement occurs commonly in the form of symmetrical distal long bone enlargement. In advanced disease, proximal long bones and flat bones of the pelvic and shoulder girdles, musculotendinous insertions, and interosseous membranes get involved. It is important to rule out secondary causes of HOA, like suppurative lung disease, carcinoma lung, congenital cyanotic heart disease, infective endocarditis, etc. Other differentials include acromegaly, thyroid acropachy, and scleromyxedema. Primary HOA usually presents with painless involvement of bones and only occasional epiphyseal involvement. The pathogenesis of primary HOA has still not been convincingly elucidated, but the most accepted theory is the platelet fragmentation theory. [6] Pulmonary microcirculation bypass (pulmonary arteriovenous shunts) leads to larger-sized platelets escaping unfragmented into the systemic circulation, leading to endothelial cell activation and release of platelet-derived growth factor (PDGF), increased expression of PDGF-BB binding sites, and enhanced PDGF-induced phosphotyrosine kinase activity, resulting in soft tissue growth causing clubbing and periostosis. It is hypothesized that in primary HOA, this also activates fibroblasts, leading to uncontrolled collagen formation, resulting in pachyderma. Myelofibrosis is believed to be caused by an overproduction of type III collagen due to PDGF, transforming growth factor- β (TGF-β), and epidermal growth factor(EGF), which are each contained within a-granules of megakaryocytes. The presence of elevated levels of von Willebrand factor in patients with cardiogenic hypertrophic osteoarthropathy, as well as in those with primary HOA, lends credence to this hypothesis. [7] Anemia in such patients is usually multi-factorial, caused by gastrointestinal bleeding, myelofibrosis, and serum inhibitors of erythropoiesis. [4],[8] Our patient also had another interesting association - that of an empty sella, which has never been reported before. In fact, one review actually suggested that primary HOA could involve virtually any bone except the carpal bones, tarsal bones, and the sella turcica. [9] References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08011f3.jpg] [ms08011f2a.jpg] [ms08011f1.jpg] [ms08011f2b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}