 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
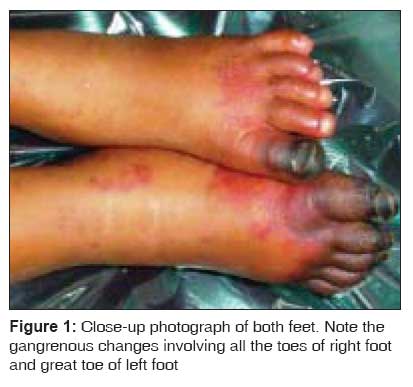
Indian Journal of Medical Sciences, Vol. 62, No. 2, February, 2008, pp. 70-73 Letter To Editor An unusual complication of Plasmodium falciparum malaria Tamhankar Parag, Tullu MilindS, Lahiri KeyaR, Deshmukh ChandrahasT Pediatric Intensive Care Unit, Department of Pediatrics, Seth G. S. Medical College and K.E.M. Hospital, Parel, Mumbai Correspondence Address:Dr. Milind S. Tullu, 'Sankalp Siddhi', Block No. 1, Ground Floor, Service Road, Kher Nagar, Bandra (East), Mumbai - 400 051, Maharashtra, India. E-mail: milindtullu@vsnl.net Code Number: ms08013 Sir, The occurrence of symmetrical peripheral gangrene (SPG) is an extremely rare entity in malarial fever (with about 18 cases reported, only 4 being children). [1],[2] A 2½-year-old girl was admitted with high-grade fever of 5 days' duration and altered consciousness (decreased activity and speech) for 2 days. She was treated elsewhere with intravenous quinine (loading dose only) and dopamine (5 µg/ kg/ min) for malarial fever complicated with shock. There she had developed blackish-blue discoloration of the fingertips, toes, tips of the earlobes; and three similar-appearing patches on the arms and legs. The ambient atmospheric temperature was warm (month of August in Mumbai, India). On arrival at our center, she was still febrile and hypotensive (BP 70/40 mmHg) with acidotic breathing. She had altered sensorium with Glasgow coma scale of 8 and exaggerated deep tendon reflexes. Firm hepatosplenomegaly (liver 3 cm palpable with span of 8 cm and spleen of 3 cm) was noted, as also pallor and icterus. Gangrenous changes were noted in distal digits of the hands and toes bilaterally [right hand: index, middle, ring fingers - distal and middle phalanges; left hand: all fingers - distal and middle phalanges, sparing the thumb; right foot: all toes affected and left foot: only great toe affected] and tips of the earlobes [Figure - 1]. Purple-bluish patches were present on the legs and arms as well. Investigations revealed hemoglobin of 6 gm%, total leukocyte count of 28,000/cmm (75% polymorphs, 25% lymphocytes) and platelets of 80,000/cmm. P. falciparum and P. vivax rings were seen (in the erythrocytes) on peripheral smear examination, the parasitic index being 90%. Venous blood gases showed uncompensated metabolic acidosis (pH 7.02, bicarbonate 10 mEq /L, base excess -6) and serum aspartate aminotransferase (140 IU/L) and indirect bilirubin (1.4 mg%) were elevated. Renal profile (blood urea nitrogen 18 mg%, serum creatinine 1.0 mg%) was normal. Doppler study of peripheral arteries showed low-amplitude signals suggestive of a vasoconstrictive etiology. 2-D echocardiography did not reveal evidence of an intracardiac thrombus. Three consecutive blood cultures were negative. Coagulation profile showed normal prothrombin time, activated partial thromboplastin time and thrombin time. However, D-dimers was strongly positive, and serum fibrinogen levels were elevated (702 mg/dl, normal 200-400 mg/dl). Anti-nuclear and anti-dsDNA antibodies were negative. Serum cryoglobulin levels were not sent owing to financial constraints. Biopsy of tissue was deferred, and the digits were allowed to auto-amputate. The patient was treated with quinine, pentoxiphylline drip (rheologic agent), intravenous piperacillin and amikacin (antimicrobials). The dopamine was discontinued and dobutamine drip was used instead. She was transfused a total of 60 cc/kg of packed red cells over a week. Limb elevation, early physiotherapy for the toes and fingers and inter-digital packing and protection from trauma were instituted. Over a period of next 1½ months, the gangrene became well demarcated, and two digits of her left hand got auto-amputated distally. She was referred for further surgical management. Symmetrical peripheral gangrene (SPG) is a rare clinical condition manifesting with acral ischemic damage in two or more extremities, without evidence of obstruction or vasculitis of the relevant artery. SPG has been reported in DIC, low cardiac output states (myocardial infarction, congestive cardiac failure, shock), malignancies (Hodgkin's disease), collagen vascular diseases (systemic lupus erythematosus), use of vasopressors (dopamine, epinephrine), reaction to drugs (sulphamethazine, penicillin) and miscellaneous causes (like coma, ergotism, acquired hemolytic anemia), etc. [3] Among the infections, meningococcal, streptococcal, E. coli, Pseudomonas, Kleibsella, proteus, viral gastroenteritis, varicella and disseminated tuberculosis are reported to cause SPG. Most of these conditions (except malaria and DIC) were excluded in our patient on the basis of clinical presentation and investigations. The basic causative factors for SPG include low cardiac output, vasospastic conditions and small-vessel obstruction. The etiological factors in our case can be explained by the triple insult of the hyperparasitemia, shock and vasospastic action of dopamine. All the cases of SPG with malaria reported in literature had evidence of DIC. Elevated D-dimers reflect the process in our patient. Heavy malarial parasitemia leads to sluggish microcirculation as parasitized red cells along with uninfected erythrocytes form microaggregates (rosettes) and attach to different endothelial cell receptors (cytoadherence). [4] Tendency to form rosettes may differ among different individuals due to host genetic differences such as complement receptor 1 polymorphisms, differences in heparin sulfate molecule type or density on the uninfected erythrocyte surface or differences in prevalence of other blood group determinants. [4] The parasites alter the lipid distribution across the red cells activating the intrinsic coagulation and the complement pathways leading to DIC. [5] Additionally, occlusion of small blood vessels with fall in the intra-luminal pressure below a certain critical value (36-60 mmHg) has been demonstrated. [6] This occurs in cases of shock and hypovolemia. [6] In our patient, the disease was arrested in the pro-coagulant phase, which left fibrin deposits in the dermal and acral capillary networks but the areas of ischemia did not extend. This process is irreversible, as barring a few cases, the gangrene leads to amputation of the digits. [7] Various treatments, viz., epoprostenol (prostacyclin), tissue plasminogen activator, [7] aspirin, vasodilators and sympathetic blockade have been suggested. [8] Such modalities, however, are generally unsatisfactory. Though used in our patient, the role of pentoxiphylline is controversial owing to its side effects like bleeding, drowsiness and hypotension. The primary treatment of this condition includes treating the underlying cause, treatment of the DIC (with heparin) to prevent extension of SPG, avoiding use of dopamine, prompt recognition and treatment of shock and preventing extension of gangrene by avoiding infection and trauma. This case is being reported for the unusual occurrence of SPG in a pediatric patient of severe malarial fever. References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08013f1.jpg] |
| |||||||||

{kind=link}