 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
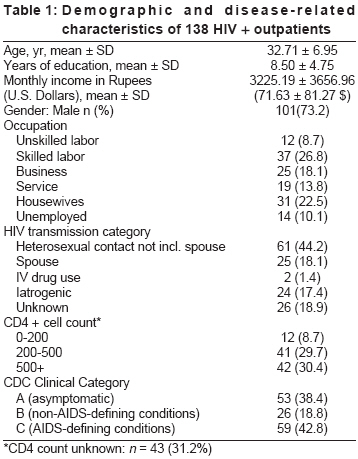
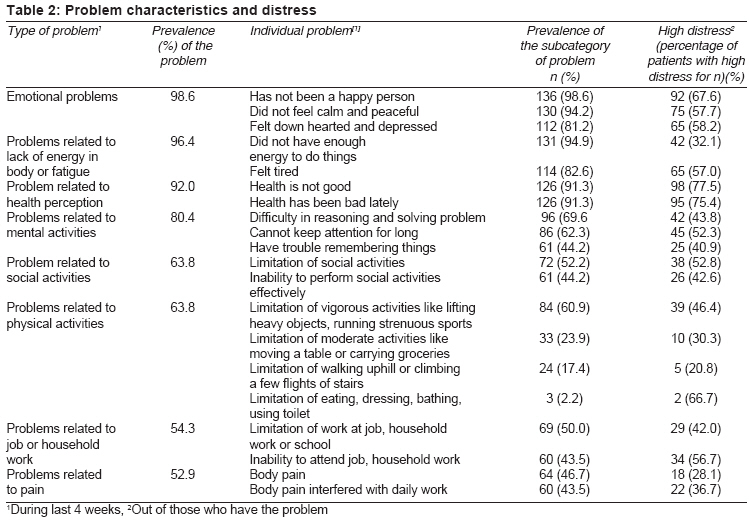
Indian Journal of Medical Sciences, Vol. 62, No. 3, March, 2008, pp. 87-97 ORIGINAL CONTRIBUTION Multidimensional health status of HIV-infected outpatients at a tertiary care center in north India Wig Naveet, Sakhuja Ankit, Agarwal SunilKumar, Khakha DeepikaC, Mehta Saurabh, Vajpayee Madhu Department of Medicine, All India Institute of Medical Sciences, New Delhi Code Number: ms08016 Abstract Background : Quality of life (QOL) scores inform researchers acquainted with such tools about patients' perception of various domains of their health. The scores provide a useful denominator for clinical trials, especially in chronic diseases with therapeutic side effects, such as HIV. However, in clinical settings, there is a felt need of description of problems commonly perceived by patients.Aim : This study describes the multidimensional health-related issues of HIV-positive patients. Settings and Design : Cross-sectional design with convenient sampling was used to recruit 138 HIV-positive patients at the outpatient section of the Department of Medicine of a tertiary care hospital in north India. Materials and Methods : A structured questionnaire was used to collect information about health-related problems. Identified problems were assessed using a Likert scale for severity. Results : Out of the 20 assessed problems, the patients reported positive for an average of 12.01 ± 3.78 problems. The most prevalent problems were those related to emotions (98.6%), lack of energy (96.4%), and health perception (92.0%). The most distressing problems were 'feeling that health was not good' (77.5%) and 'health was bad' (75.4%). The number of problems reported was significantly related to weight loss ( P = 0.006) and clinical category ( P = 0.023). A significant correlation was observed between weight loss and problems in social activities ( P < 0.001), pain ( P < 0.001); clinical class ( P < 0.001); tuberculosis, and problems in job and household work ( P = 0.002). Conclusion : Many patients have significant problems in dimensions other than physical. A physician's awareness about these problems is important for a holistic patient management. Keywords: HIV, India, multidimensional health status, quality of life Introduction With more than 5.1 million human immunodeficiency virus (HIV)-positive patients, India has the second highest number of people living with HIV. [1] Improvement in life expectancy for people living with HIV and AIDS (PLHA) has resulted in greater emphasis on ways to improve quality of life. [2] As a result of increased longevity, PLHA have to deal with more than just disease-related morbidities, such as side (and adverse) effects of drugs, social challenges, psychological and economic stress. No illness exists in a vacuum. [3] One way of capturing personal and social context of patients is to use quality of life measures. Quality of life (QOL) is a complex construct with operational difficulty in both its assessment and interpretation. However, it provides a useful tool for capturing the complex scenario. Clinical and biological end points used during pharmacological trials (CD4 level, viral load, opportunistic diseases) are considered inadequate to catch the complexity of care and treatment outcomes. [4],[5] Hence, QOL is currently considered essential while evaluating clinical trials. [4] Many instruments are used to access the QOL of HIV patients. Some of these were developed specifically for HIV patients, and others are generic. Some examples are multiple versions of Medical Outcome Study (MOS). [6],[7],[8],[9],[10],[11],[12],[13],[14],[15] We have used The World Health Organization Quality of Life (WHOQOL)-BREF [16],[17] for measuring quality of life in 68 HIV patients in the same setup. [18] It provides scores on a scale of 0 to 100, which is often useful for assessing the outcome of a therapy in patients on follow-up. Existing HRQOL assessment tools exclude several aspects relevant in clinical settings as they are mainly designed for research and clinical trials. [19] However, such scores provide little information to the treating physicians about health-related problems of PLHA. There is no published study from India that provides physicians a comprehensive picture of the problems faced by patients in other domains of health and the perceived severity of such problems. The aim of this study was to describe the multidimensional health-related issues in a sample of PLHA in north India. The study attempts to inform physicians about such problems rather than develop a new QOL assessment tool. Materials and Methods Study design: Cross-sectional Study duration: Eleven months (July 2001 to May 2002) Measures History and physical examination: A detailed medical history of the patients, along with a meticulous physical examination, was done. Lab investigations: Cluster differentiation 4 (CD4) lymphocyte count was determined as a routine investigation and served as the main criterion of immunity status. We also inquired about the mode of transmission after proper counseling to know the probable mode of transmission. The standard Center for Disease Control (CDC) guidelines were followed for characterizing subjects into various HIV categories (clinical categories A, B, C; and CD4+ count categories 1, 2, 3). Measuring multiple dimensions of health Statistical analyses Results Sample characteristics The mean body mass index (BMI) was 19.32 ± 3.48 kg/m 2 (range, 11.7-29.2). The mean CD4 count was 278 ± 221 (range, 15-1577). Total subjects in CD4 category III were 42 (30.43%), and the number of subjects in CDC clinical category C was 59 (42.8%). The mean hemoglobin level was 11.26 ± 2.38 mg/dL (range, 5-16), and the mean lymphocyte count as a percentage of the total leukocyte count was 31.70 ± 8.08 (range, 9-55). The number of patients suffering from active tuberculosis at the time of initial evaluation was 55 (39.9%); the distribution of the types of tuberculosis among them was as follows: pulmonary tuberculosis, 40 (72.72%); disseminated tuberculosis, 36 (65.45%), and extra-pulmonary tuberculosis, 13 (23.64%). Among other HIV-associated illnesses, 30 (21.7%) had oral candidiasis, 27 (19.6%) had persistent diarrhea, and 4 (2.9%) had pneumocystis carinii pneumonia. Problem characteristics and distress Among the eight areas assessed, emotional problems took the lead with 136 (98.6%) of patients reporting it. It was followed by problems related to lack of energy in the body or fatigue, 133 (96.4%); and problems related to health perception, 127(92.0%). The least prevalent problems were those involving physical activities, 88 (63.8%); problems in job and household work, 75 (54.3%); and problems due to pain, 73 (52.9%). As of individual problems, 136 (98.6%) of the subjects did not think they were happy individuals in the preceding 4 weeks. Out of these, 92 (67.6%) considered themselves unhappy most of the time during the preceding 4-week period. Almost all, 131 (94.9%) of the subjects, did not have enough energy to do things they wanted to do during the preceding 4 weeks; also, 42 (32.1%) of these reported severe lack of energy. Some other common individual problems were ′not feeling calm and peaceful′ (94.2%), ′not having a feeling of good health′ (91.3%), and ′feeling that health had been bad lately′ (91.3%). The least prevalent problems were eating, dressing, bathing or using a toilet, 3 (2.2%); walking uphill or climbing a few flights of stairs, 24 (17.4%); moderate activities like moving a table or carrying groceries, 33 (23.9%); absenteeism at job because of health, 60 (43.5%); and suffering due to pain in the body, 60 (43.5%) [Table - 2]. Among the positive problems, the high-distress problems were those related to perception of health - ′feeling that their health was not good′ was the most distressing problem, with 98 (77.5%) patients experiencing this problem; it was closely followed by ′feeling that their health was bad lately,′ with 95 (75.4%) patients experiencing high distress. Some of the other highly distressing problems were as follows: ′not feeling calm and peaceful′ was a source of high distress in 75 (57.7%) patients; ′feeling tired′ was reported by 65 (57.0%) patients; and ′inability to attend place of job, school, or household work due to poor health′ was a source of high distress in 34 (56.7%) patients of the problem-positive patients. Some of the least distressing problems reported were problems in walking uphill or climbing a few flights of stairs, problems in moderate activities like moving a table or carrying groceries, and lack of enough energy to do things they wanted to do. Correlates of problem prevalence, distress levels with socio-demographic, clinical and laboratory parameters Analysis showed no significant difference in the number of problems reported or distress levels for individual problems between men and women. A significant correlation was observed between the number of problems and weight loss (P = 0.006); and number of problems and clinical category of the disease (P = 0.023). No significant difference was observed in individual symptoms or distress with varying age or educational status, transmission category or CD4 category. A significant correlation was observed between active tuberculosis and problems in job or household work (P = 0.016), as also between active tuberculosis and a feeling of lack of energy (P = 0.033). Active tuberculosis also significantly affected social activities (P = 0.013). A history of tuberculosis was significantly correlated with problems at job and household work (P = 0.002), social activities (P = 0.042), and physical activities (P = 0.042). Age had a mild correlation with physical problems (P = 0.047); social problems (P = 0.021); with more physical and social problems seen with increasing age. We found that men had more problems in social activities than women (P = 0.025). Weight loss was significantly associated with social problems (P < 0.001), pain (P < 0.001), problems in job and household work (P = 0.005), problems in physical work (P = 0.005), and problems related to health perception (P = 0.047). BMI was found to be significantly associated with a feeling of lack of energy in the body (P = 0.025), problems involving mental exercise (P = 0.017), social activities (P = 0.030), and physical activities (P = 0.040). Anti-tubercular therapy (ATT) was significantly associated with problems in social activities (P = 0.033), with those taking ATT having more problems; and it was also significantly associated with problems in job and household work (P = 0.005), with those taking ATT having more problems. Antiretroviral therapy (ART) had a mild but statistically significant correlation with problems of health perception (P = 0.047), with only 5.6% of those not on ART having no such problems as opposed to 16.7% of those on ART. We also found a significant correlation between transmission category and symptoms of lack of energy in the body (P = 0.028). Social problems were more common in those with clinical class C disease as compared to those with class A disease (83.1% vs. 43.4%; P < 0.001). Similarly, 64.4% of patients in class C had problems because of pain as compared to only 35.8% of patients in class A (P = 0.006). Limitations Discussion With increasing prevalence of HIV (owing to increased longevity adding to increasing incidence) and free ART availability, physicians will encounter more HIV-positive patients. This study describes the multidimensional health issues that might concern PLHA. The major mode of HIV transmission in India is through sexual contact, responsible for 85.34% of cases. Blood products account for 2.05%; IV drug use, 2.34%; perinatal transmission, 3.80%; and others (not specified), 6.46%. [20] In our study, heterosexual contact was responsible for 44.2% of cases, blood products for 17.4%, IV drug use for 1.4%, and other causes for 15.2% of the cases. The discordance is similar to one found in our previous study, [18] showing the difference in the number of patients self-reporting due to various factors such as stigma attached and guilt of heterosexual contact outside marriage. In our study, emotional problems were the most prevalent ones (98.6%). HIV/AIDS has been associated with emotional problems in other studies also [21],[22],[23],[24] HIV not just affects an individual but the whole family. [25] Lack of mental peace and depression widely affect the quality of life and day-to-day functioning of a person [23] and may even lead to failure of HAART. [26] Therefore, it is important for physicians to address this problem using the available treatment options. [27] The second most prevalent problem was that of lack of energy in the body, or fatigue (96.4%). Other studies have also reported it to be one of the common problems. [22],[28],[29],[30] Fatigue has a multifactorial origin [22],[29],[31] that includes lack of rest or exercise, improper or inadequate diet, psychological stress, anemia, infection, thyroid abnormalities, side effects of medication, sleep disturbances, and fever. Fatigue has not been found to correlate with CD4 counts, [31],[32] and this was seen in our study. It is to be noted that CD4 counts for 31.2% of patients included in the study were unavailable, and this could have influenced the results. The most prevalent problems of our study - fatigue and emotional problems - often coexist and are interrelated. [29] Many physiological markers and psychological constructs are available for objective assessment of fatigue. [31],[33] There is a need for routine assessment and management of fatigue in patients with HIV. [34] There are currently no clear guidelines available for clinicians who treat HIV-infected patients experiencing fatigue. A number of therapies have been tried, including supplements, vitamins, nutrition, sleep, rest, exercise, and approaches like thought distractions, [35],[36] dehydroepiandrosterone (DHEA), anabolic steroids and testosterone therapy, [36],[37],[38],[39],[40],[41] antidepressants, [36] hydrocortisone, epoientin alfa, [36],[38] dextroamphetamine, [42],[43] and hyperbaric oxygen therapy. [44] Physicians should seek the underlying treatable causes of fatigue and treat these conditions. [32] The third common and most distressing problem was related to perception of health (92.0%). Problems related to perception of health have been addressed earlier also. [45] Patients′ health perception and way of coping have been shown to influence their immune responses. [46],[47] Problems related to pain were the least reported in our study (52.9%). Pain has been associated with depression, anxiety, and suicidal ideation. [24] Individuals with persistent pain are known to be at heightened risk for posttraumatic stress disorder (PTSD). [48] Despite these facts, pain is one of the factors most overlooked by physicians. [22] Thus, physicians need to be aware and forthcoming in asking about, and treating, pain in order to improve a patient′s overall health. Weight loss was associated with a number of problems such as social problems, problems related to pain, problems in job and household work, and problems in performing physical work. Weight loss is a negative prognostic indicator in PLHA. [49] Weight loss is often associated with anorexia. [50] Multiple treatment options are available for treatment of weight loss. [50],[51],[52],[53] Tuberculosis is the most frequent opportunistic infection in HIV patients in India (54% of all AIDS patients). It is estimated that 2.6% to 8% of tuberculosis patients in India are HIV infected. [54],[55] A significant correlation between active tuberculosis and lack of energy in the body, problems in job or household work, and problems in social activities was observed. The questionnaire used here has not been validated with other existing tools, but its value lies in simplicity and in increasing awareness among health care providers in the Indian context. Conclusions Problems related to emotions and fatigue were the most prevalent ones, whereas those related to pain and physical problems were among the least prevalent ones. The most distressing problems were those related to health perception. Thus, this study demonstrates that HIV-positive patients have problems in various aspects of life, other than those assessed in a busy clinic. Attention towards these problems would be beneficial for holistic patient care. References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08016t1.jpg] [ms08016t2.jpg] |
| |||||||||

{kind=link}
{kind=link}