
|
Indian Journal of Medical Sciences
Medknow Publications on behalf of Indian Journal of Medical Sciences Trust
ISSN: 0019-5359 EISSN: 1998-3654
Vol. 62, Num. 3, 2008, pp. 105-112
|
Indian Journal of Medical Sciences, Vol. 62, No. 3, March, 2008, pp. 105-112
ORIGINAL CONTRIBUTION
Apolipoprotein E polymorphism and its relation to plasma lipids in coronary heart disease
Singh PP, Singh M, Bhatnagar DP, Kaur TP, Gaur SK
Molecular Genetics Laboratory, Department of Human Biology, Punjabi University, Patiala
Correspondence Address:Molecular Genetics Laboratory, Department of Human Biology, Punjabi University, Patiala - 147 002, Punjab,
singh.puneet@rediffmail.com
Code Number: ms08018
Abstract
Background : The present investigation is aimed at examining the Apolipoprotein E (APOE) genotypic influence on coronary heart disease (CHD) risk in northwest India (Punjab), where this disease is emerging as a major threat to public-health care system.
Materials and Methods: The present study comprised of angiographically diagnosed coronary heart disease patients (n = 193) and controls (n = 150) of Punjab. Genetic polymorphism of APOE gene was investigated by polymerase chain reaction (PCR), and its association with lipid levels was evaluated.
Results : The allele frequencies of ε2, ε3, and ε4 were 0.054, 0.795, 0.151; and 0.077, 0.856, 0.067 in patients and controls respectively. The bearers of E3/E4 genotype had threefold higher propensity of developing CHD in this population (OR, 3.04; CI, 1.55-6.25; P < 0.001), which exacerbated (OR, 4.18; CI, 2.03-9.27; P < 0.001) after correcting for age, sex, BMI, and lipid-lowering drugs. Lower HDL-C levels and higher LDL-C levels were found to be correlated with E3/E4 genotype (P < 0.01). Other concomitants like body mass index (BMI), total cholesterol (TC), and triglyceride (TG) levels did not show up as genetic determinants in this part of the region.
Conclusions : A significant association (P = 0.016) of ε4 allele, especially E3/E4 genotype, with CHD was observed, along with HDL-C and LDL-C concentrations, in the population of northwest India.
Keywords: APOE, APOE polymorphism, Apolipoprotein E, coronary heart disease, Punjab
Introduction
The burden of coronary heart disease (CHD) is posing a huge threat to the public health system, especially in developing countries like India [1] and to the immigrant Asian Indians as compared to other ethnic groups. [2] In India, especially in Punjab, after 30 years of age, 31% of the total diseased are coronary heart patients. [3] Besides other known candidates of coronary heart diseases, Apolipoprotein E (APOE) has also been recognized as a potential genetic marker for CHD. [4],[5],[6]
Apolipoprotein E plays an imperative role in the secretion, processing, and metabolism of various lipoprotein particles across cell membranes in systemic and cerebrospinal systems through reverse cholesterol transport in the body. [7] The APOE gene is localized on 19q13.2 in an approximately 45 kb gene cluster containing the genes for APO CI, CII, CIV, and CI pseudogene, along with elements controlling their tissue-specific transcription. [8] Two SNPs in position 3937 and 4075 in exon 4 result in three common alleles ε2, ε3, and ε4, differing in amino acid substitution of cysteine to arginine at codon 112 and 158, which lead to variations in the binding affinity of resultant genotype for APOE and LDL receptor, [9] LDL formation rate, and cholesterol absorption. [10] In lieu of these variations, triglyceride (TG), high-density lipoprotein (HDL), and low-density lipoprotein (LDL) metabolism becomes defective and augments the conditions for the development of atherosclerosis and coronary heart disease. [11],[12]
Some reports have heralded various relationships of APOE genotypes vis-à-vis lipid parameters, ethnicity, environment, and gene-diet interactions in CHDs. [13],[14],[15] Therefore, the present study is conducted to investigate the APOE gene polymorphism in CHD patients of Punjab. Its relationship with lipids and lipoprotein levels is also examined, which has not been done in this region hitherto.
Materials and Methods
Study subjects
The population in the present study comprised of 193 angiographically diagnosed coronary heart disease patients and 150 healthy control subjects. All the patients and controls gave their written consent prior to participation, and the study procedures followed were in accordance with the institutional ethical committee′s guidelines. The patients ranging in age from 45 to 65 years (mean age 54.94 ± 11.43) were selected from the outpatient clinics and wards of two hospitals of Punjab. Only those patients who had> 50% stenosis in any of the three major coronary arteries were included. All control subjects (males, 105; females, 45; mean age, 53.42 ± 12.47 years) were with normal electrocardiograms, a fact that was verified by the physician using Minnesota codings [15] and cardiovascular Rose questionnaire. [16] The patients and controls included in the present study were unrelated and belonged to Punjab (northwest India). Predisposing factors for CHD, like family history, hypertension (systolic blood pressure/diastolic blood pressure ≥140/90 mm Hg), diabetes, smoking (current smoking, 10 cigarettes a day), and alcohol use (>200 mL/day for at least 6 days in a week), were determined through interaction with the patients or from their clinical records. Some of the patients (58.55%) were taking lipid-lowering drugs like fibrates and statins. Blood pressure was measured with the subjects in supine position. Diabetes was considered if the subject was being treated for diabetes at the time of sampling. The family history of CHD was considered positive on the basis of death of mother or father due to myocardial infarction, CHD, or stroke. Height and weight of subjects were taken with light clothing, and body mass index (BMI) was calculated according to the Quetelet equation (BMI = weight in kilograms/height in meters squared). Subjects taking hormone replacement therapy (HRT) and other hormonal drugs were not included. Those subjects who had renal and hepatic insufficiency were also excluded.
Lipid analysis
Blood was drawn from antecubital vein into EDTA (5 mg/mL) tubes after an overnight fast. Lipid profiles were determined immediately from freshly separated plasma. Total cholesterol, high-density lipoprotein cholesterol, and triglycerides were measured by one-step method using commercially available kits (Span Diagnostic and Erba Mannheim). The coefficient of variation for these measurements was less than 1.6%. LDL cholesterol was calculated by Freidewald equation up to TG < 400 mg/dL. [17]
APOE genotyping
Genomic DNA was extracted with the standard phenol chloroform extraction method. All genotyping was done without the knowledge of case/control status of each study individual. The APOE genotypes were deduced by polymerase chain reaction (PCR) using oligonucleotide primers (Hysel India Ltd.), forward primer, 5′-ACA GAA TTC GCC CCG GCC TGG TAC AC-3′, reverse primer, 5′-TAA GCT TGG CAC GGC TGT CCA AGG A-3′. [18] The amplified DNA fragments were separated on 3% agarose gels as described previously. [19] Amplicons were recognized using pBR 322 DNA-MspI digest as bp marker (Bangalore Genei). Internal validation of the polymorphism was done by re-analyzing some samples to avoid bias in genotyping error. 224 bp amplicon digested with HhaI resulted in six APOE genotypes, viz., E2/E2 (91, 81, 38,19), E3/E3 (91, 48, 38, 33), E4/E4 (72, 48, 38, 33), E2/E3 (91, 81, 48, 38), E2/E4 (91, 83, 72, 48, 33), and E3/E4 (91, 72, 48, 38, 33).
Statistical analyses
Clinical data were expressed as mean ± SD, and the differences between patients and controls were analyzed by t-tests for continuous variables and χ2 tests for categorical concomitants. Allele frequencies were estimated by gene-counting method. Chi-square test was used to investigate the differences between observed and expected genotype frequencies assuming Hardy-Weinberg equilibrium, and differences in allele frequencies of CHD patients and controls as well. Odds ratio (OR) with 95% confidence intervals and P values were calculated for examining the association of APOE genotypes in both the groups. To investigate the independent contribution of the Apolipoprotein E polymorphism to the levels of lipid variables, the lipid values were adjusted for sex, age, BMI, and lipid-lowering drugs using multiple linear regression (GLM procedure). As the TG values were skewed, log-transformed values were used for analysis. Lipid and lipoprotein values in patients and controls were compared using the two-sample students ′t′ test. One-way analysis of variance (ANOVA) was performed taking E3/E3 as reference. (E2/4 and E4/4 were merged with E3/E4, and E2/E2 was merged with E2/E3.) EXCEL and SPSS (V.12, SPSS, Chicago) were used for statistical analysis. A two-tailed P value less than 0.05 was considered significant within and between variables.
Results
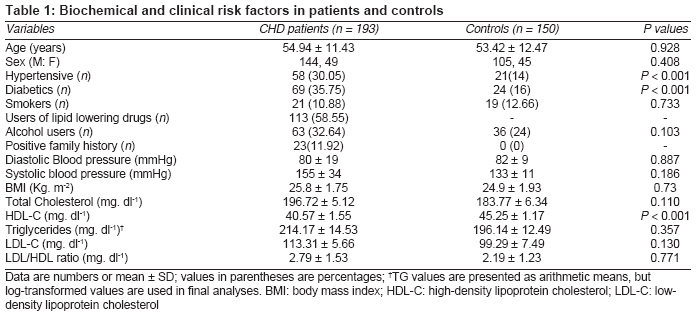
The clinical and biochemical characteristics of patients and controls are presented in [Table - 1]. The age range of the patient and control groups was 45 to 65 years (mean age, 54.94 ± 11.43 years and 53.42 ± 12.47 years respectively). The allele frequencies of both patients and controls were found to be in Hardy-Weinberg equilibrium (P > 0.05). Twenty-three (11.92%) patients showed positive family history. As expected, diabetics and hypertensives were more common in the patient group as compared to controls, and the difference was significant (P < 0.001); however, the differences in means of diastolic and systolic blood pressure were trivial. The impact of smoking, alcohol, and BMI was observed to be small in both the groups. Patients had significantly decreased high-density lipoprotein cholesterol levels than controls (40.57 vs. 45.25, P < 0.001).
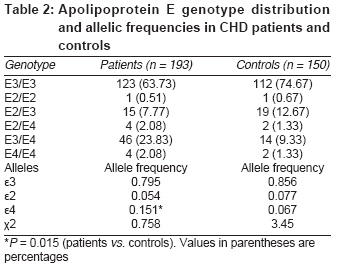
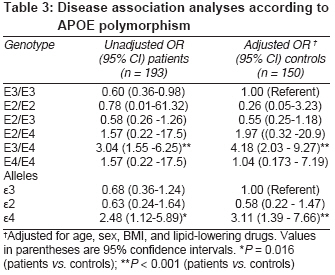
[Table - 2] illustrates that ε3 allele (>80%) and E3/E3 genotypes were the most common in both the groups, which is consistent with the ε3 allele frequency value found in Caucasians and Indians. [20] ε4 carriers were observed to be more common in patients than in controls. The variation of E3/E4 genotype and ε4 allele frequencies was found to be significant in both the groups (P = 0.015). Disease association analysis [Table - 3] showed that the carriers of ε4 allele and especially E3/E4 genotypes were portending higher risks of CHD (ORs, 2.48 and 3.04 respectively; P = 0.016), which exacerbated (ORs, 3.11 and 4.18 respectively; P < 0.001) after correcting it for age, sex, BMI, and lipid-lowering drugs.
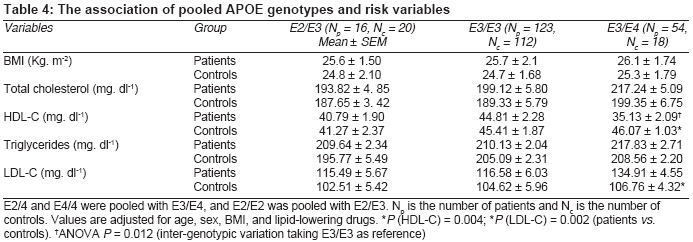
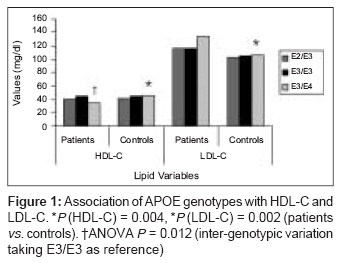
To investigate the genetic association of APOE polymorphism with CHD, values of lipids, along with BMI, were categorized according to the APOE genotypes [Table - 4]. Separate comparisons of systolic and diastolic blood pressure according to APOE genotypes showed insignificant variation. No sex-specific differences in lipid levels according to APOE genotype were evident (data not given). Moreover, the lesser number of females in comparison to males could not substantiate it. HDL-C was found to be depressed noticeably in patients having E3/E4 genotype than in controls (P = 0.004). Similarly, variation in LDL-C at E3/E4 genotype was found to be statistically significant (P = 0.002) in both the groups [Figure - 1]. Other variables like body mass index, total cholesterol, and triglyceride concentrations were not observed to be the genetic determinants in CHD. Significant inter-genotypic variation in patients having E3/E3 and E3/E4 genotype was noticeable for HDL-C (F = 1.912, P = 0.012).
Discussion
The present study investigated the role of APOE gene polymorphism and its association with lipid and lipoprotein levels in angiographically verified coronary heart disease patients of Punjab (northwest India). It was found that the carriers of ε4 allele, especially E3/E4 genotype, had a 4.2-fold higher risk of CHD in this population after adjustment for age, sex, BMI, and lipid-lowering drugs. Considerable variation in ε4 allele frequency was observed (P = 0.015) in both the groups, which was in accordance with many studies conducted in different regions with varied prevalence of CHD; [5],[21],[22],[23] however, some studies failed to show such association. [24],[25] The reasons for the inconsistent association of CHD with APOE polymorphism probably are inter-ethnic diversity [11],[20] and environmental factors. [26],[27]
Since APOE varies according to age and sex, multiple linear regression was applied and lipid values were adjusted for these variables. The findings of low levels of HDL-C in E3/E4 genotype in patients were in agreement with those of other studies on different populations, [5],[12] as well as north Indian CHD patients. [28] In the present study, patients having E3/E4 genotype had higher mean LDL-C than controls (P = 0.002). Besides probable APOE gene-diet interactions, it was expected because of the different binding affinities of APOE isoforms to LDL and chylomicron receptors.
Marginally higher TC and TG levels were noticed in CHD patients having E3/E4 and E2/E3 genotype when compared with controls but the differences were insignificant. The influence of APOE polymorphism on plasma lipids and lipoproteins varies according to ethnicity and is even absent in some populations. In addition, some local mechanisms like urbanization, sedentary life style, and increased consumption of high-fat and low-fiber diet might be attributable to these differences. Punjab is considered as the high saturated fat-consuming belt of the country. The presence of low levels of TC and TG in patients and controls further suggested that for these lipids, homeostatic mechanism-controlling lipid distribution in APOE genotypes and their metabolism operate efficiently in this part. It is believed that APOE umpires its adverse or protective actions via several crucial mechanisms and factors like ethnicity, age, environment, affiliated diseases, and gene-diet interactions.
In conclusion, this investigation on the Punjabi coronary heart disease patients and controls found a significant association of APOE genotypes with high- and low-density lipoprotein cholesterols. In addition, the strong influence of ε4 allele and E3/E4 genotype as the risk markers of CHD was revealed.
Limitations of the study
Although this study is descriptive, it has some limitations, like the association of APOE gene with CHD could be categorized according to CHD subtypes such as stable coronary artery disease (CAD), acute myocardial infarction (AMI), etc.; but as no other study on APOE gene polymorphism vis-à-vis CHD has been reported from Punjab, its importance cannot be underrated. Moreover, with that study design, it would have given less robust statistical inferences with the same sample size. Although we have adjusted the effects of all the potential confounding variables, we may have missed some factors inadvertently, such as socioeconomic status, nutritional factors which would have influenced the disease status, but the bias might have been balanced as all the major region-specific predisposing factors are included. The interpretations cannot be generalized for the entire northwest region because of the limited data and cross-sectional design of the study.
Acknowledgments
I owe my sincere thanks to Drs. Inder Johal, Amrit Randhawa, Saravpreet Grewal, Kanwalpreet Singh, and the paramedical staff, all of whom have been greatly helpful in the process of data collection and assimilating the affiliated information. Thanks are also due to CSIR and DST for conferring designations of Research Associate and Scientist to the authors PPS and MS respectively, without which this work would have been ineffectual.
References
| 1. | Reddy KS, Yusuf S. Emerging epidemic of cardiovascular disease in developing countries. Circulation 1998;97:596-601. Back to cited text no. 1 |
| 2. | Hughes K, Aw TC, Kuperan P, Choo M. Central obesity, insulin resistance, syndrome X, lipoprotein (a) and cardiovascular risk in Indians, Malays and Chinese in Singapore. J Epidemiol Community Health 1997;51:394-9. Back to cited text no. 2 |
| 3. | Wander GS, Khurana SB, Gulati R, Sachar RK, Gupta RK, Khurana S, et al. Epidemiology of coronary heart disease in a rural Punjab population-prevalence and correlation with various risk factors. Indian Heart J 1994;46:319-23. Back to cited text no. 3 |
| 4. | Wang XL, McCredie RM, Wilcken DE. Polymorphisms of the apolipoprotein E gene and severity of coronary artery disease defined by angiography. Arterioscler Thromb Vasc Biol 1995;15:1030-4. Back to cited text no. 4 |
| 5. | Stengεrd JH, Zerba KE, Pekkanen J, Ehnholm C, Nissinen A, Sing CF. Apolipoprotein E polymorphism predicts death from coronary heart disease in a longitudinal study of elderly Finnish men. Circulation 1995;91:265-9. Back to cited text no. 5 |
| 6. | Wilson PW, Schaefer EJ, Larson MG ordovas JM. Apolipoprotein E alleles and risk of coronary artery disease: A meta analysis. Arterioscler Thromb Vasc Biol 1996;16:1250-5. Back to cited text no. 6 |
| 7. | Mahley RW, Huang Y, Weisgraber KH. Putting cholesterol in its place: ApoE and reverse cholesterol transport. J Clin Invest 2006;116:1226-9. Back to cited text no. 7 |
| 8. | Allan CM, Walker D, Segrest JP, Taylor JM. Identification and characterization of a new human gene (APOC4) in the apolipoprotein E, C-I and C-II gene locus. Genomics 1995;28:291-300. Back to cited text no. 8 |
| 9. | Hui DY, Innerarity TL, Milne RW, Marcel YL, Mahley RW. Binding of chylomicron remnants and beta-very low density lipoproteins to hepatic and extra hepatic lipoprotein receptors: A process independent of apolipoprotein B48. J Biol Chem 1984;259:15060-8. Back to cited text no. 9 |
| 10. | Sing CF, Davignon J. Role of Apolipoprotein E polymorphism in determining normal plasma lipid and lipoprotein variation. Am J Hum Genet 1985;37:268-85. Back to cited text no. 10 |
| 11. | Lusis AJ. Atherosclerosis. Nature 2000;407:233-41. Back to cited text no. 11 |
| 12. | Dallongeville J, Lussier-cacan S, Davignon J. Modulation of plasma triglyceride levels by apoE phenotype: A meta analysis. J Lipid Res 1992;33:447-54. Back to cited text no. 12 |
| 13. | Singh P, Singh M, Gerdes U, Mastana SS. Apolipoprotein E polymorphism in India: High APOE*E3 allele frequency in Ramgarhia of Punjab. Anthrop Anz 2001;59:27-34. Back to cited text no. 13 |
| 14. | Singh PP, Singh M, Mastana SS. Genetic variation of apolipoproteins in North Indians. Hum Biol 2002;74:673-82. Back to cited text no. 14 |
| 15. | Prineas JR, Crow RS, Blackburn H. The Minnesota code manual of electrocardiographic findings. John Wright PSG Inc: Boston, Bristol, London; 1982. Back to cited text no. 15 |
| 16. | Rose GA, Blackburn H, Gillium FF, Prineas RJ. Cardiovascular survey methods. WHO: Geneva; 1982. Back to cited text no. 16 |
| 17. | Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without the use of preparative ultracentrifuge. Clin Chem 1972;18:499-502. Back to cited text no. 17 |
| 18. | Hixson JE, Vernier DT. Restriction isotyping of human apolipoprotein E by gene amplification and cleavage with HhaI. J Lipid Res 1990;31:545-8. Back to cited text no. 18 |
| 19. | Singh PP, Naz I, Gilmour A, Singh M, Mastana S. Association of APOE (HhaI) and ACE (I/D) gene polymorphism with type 2 diabetes mellitus in North West India. Diab Res Clin Pract 2006;74:95-102. Back to cited text no. 19 |
| 20. | Singh PP, Singh M, Mastana SS. APOE distribution in world populations with new data from India and the UK. Ann Hum Biol 2006;33:279-308. Back to cited text no. 20 |
| 21. | Kuusi T, Nieminen MS, Ehnholm C, Yki-Jarvinen H, Valle M, Nikkila EA, et al. Apoprotein E polymorphism and coronary artery disease. Increased prevalence of apolipoprotein E-4 in angiographically verified coronary patients. Arteriosclerosis 1989;9:237-41. Back to cited text no. 21 |
| 22. | Corbo RM, Vilardo T, Ruggeri M, Gemma AT, Scacchi R. Apolipoprotein E genotype and plasma levels in coronary artery disease: A case-control study in the Italian population. Clin Biochem 1999;32:217-22. Back to cited text no. 22 |
| 23. | Lahoz C, Schaefer EJ, Cupples LA, Wilson PW, Levy D, Osgood D, et al. Apolipoprotein E genotype and cardiovascular disease in the Framingham Heart Study. Atherosclerosis 2001;154:529-37. Back to cited text no. 23 |
| 24. | de Knijff P, Jansen H, Lie KI, Havekes LM. Apolipoprotein epsilon 4 and coronary artery disease. Lancet 1992;340:1351. Back to cited text no. 24 |
| 25. | Damaraju S, Yu QT, Safavi F, Marian AJ. Apolipoprotein epsilon 4 is not a genetic risk factor for coronary artery disease or restenosis after percutaneous transluminal coronary angioplasty. Am J Cardiol 1995;75:1181-5. Back to cited text no. 25 |
| 26. | Corbo RM, Scacchi R. Apolipoprotein E (APOE) allele distribution in the world: Is ApoE*4 a 'thrifty' allele? Ann Hum Genet 1999;63:301-10. Back to cited text no. 26 |
| 27. | Gerdes LU. The common polymorphism of Apolipoprotein E: Geographical aspects and new pathophysiological relations. Clin Chem Lab Med 2003;41:628-31. Back to cited text no. 27 |
| 28. | Luthra K, Bharghav B, Chabbra S, Das N, Misra A, Agarwal DP, et al. Apolipoprotein E polymorphism in Northern Indian patients with coronary heart disease: Phenotype distribution and relation to serum lipids and lipoproteins. Mol Cell Biochem 2002;232:97-102. Back to cited text no. 28 |
Copyright 2008 - Indian Journal of Medical Sciences
The following images related to this document are available:
Photo images
[ms08018t3.jpg]
[ms08018t4.jpg]
[ms08018t1.jpg]
[ms08018t2.jpg]
[ms08018f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}