 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
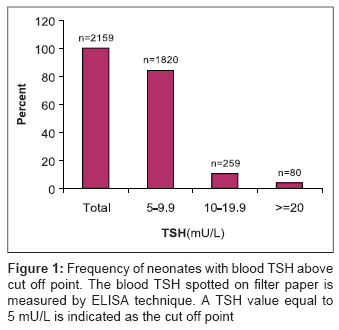
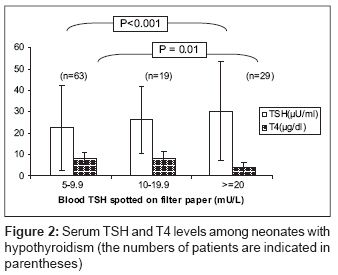
Indian Journal of Medical Sciences, Vol. 62, No. 3, March, 2008, pp. 113-116 ORIGINAL CONTRIBUTION Neonatal thyroid screening in a mild iodine deficiency endemic area in Iran Najafi Mohammad, Khodaee GholamHossein, Bahari Mohammad, Sabahi Masoumeh, Farsi MostafaMazlom, Kiani Fatomeh Central Laboratory, Health Ministry, Mashhad University of Medical Sciences, Khorasan Code Number: ms08019 Abstract Background : Evaluated serum thyroid-stimulating hormone (TSH), as an early index for diagnosis of neonatal hypothyroidism, indicates insufficient supply of thyroid hormones.Objective : The aim of the study was to estimate the incidence of neonatal hypothyroidism and assessment of iodine deficiency in the eastern part of Iran. Settings and Design : A cross-sectional study was conducted in a pilot screening. Materials and Methods : The measurement of blood TSH spotted on filter paper was performed by ELISA method in 59,436 neonates. TSH value equal to 5 mU/L was considered cut off point. The diagnosis of hypothyroidism in neonates with the blood TSH higher than the cut off point was based on clinical examinations and laboratory tests (serum TSH and T4). Statistical Analysis: The groups were compared using chi-square and ANOVA tests. Results : In our study, the recall rate and incidence of hypothyroidism were 3.6% and 2 per 1000 neonates respectively. Based on the proposal made by WHO/UNICEF/ICCIDD, the results of our study showed a mild iodine deficiency in the area. Conclusions : A comprehensive policy should be developed for control of iodine deficiency and treatment of hypothyroidism in the studied population and neighboring countries. Keywords: Filter paper, neonatal hypothyroidism, thyroid-stimulating hormone Introduction Neonatal thyroid screening is considered a monitoring tool for the early detection and therapy of hypothyroidism. [1],[2] Clinical diagnosis occurs in below 5% of neonates with hypothyroidism; thus, neonatal thyroid screening is essential as early as possible for prevention of brain damage. [3] Elevated serum thyroid-stimulating hormone (TSH) may be due to congenital hypothyroidism or iodine deficiency. [4] Both conditions can result in mental retardation. [5] The World Health Organization (WHO), United Nations International Children′s Emergency Fund (UNICEF), and International Council for Control of Iodine Deficiency Disorders (ICCIDD) have made a proposal for assessing iodine deficiency disorders (IDD). In a condition of adequate iodine intake, the frequency of neonatal TSH above cut off point (5 mU/L) is below or around 3%. [6] The present study is a pilot screening carried out in the eastern part of Iran. We evaluated the incidence of hypothyroidism and iodine deficiency in the area. Materials and Methods We screened 59,436 neonates between May 2006 and February 2007. Blood specimens in the period between the third and seventh days of life were collected on a filter paper (Schleicher and Schuell, NO 903) by heel stick and transported to a central laboratory. Based on the protocol made by WHO/UNICEF/ICCIDD, [6] low-birth weight (< 2,000 g), twin, and high-birth weight (>4,500 g) neonates were rechecked after 1 week. The blood TSH spotted on filter paper was measured by ELISA technique (Stat-Fax 2600) using neonatal TSH kit (Kima Pajouhan Co., Tehran, Iran). The inter-assay and intra-assay variations were 10.7% (TSH = 7 mU/L) and 11.8% (TSH = 5 mU/L) respectively. The blood TSH values with deviations equal to ± SDxC/M [C = cut off point, SD = standard deviation, and M = mean calculated for three standard samples] around the cut off point were rechecked at all assay runs. A TSH value equal to 5 mU/L was used as a cut off point. Neonates with the blood TSH above the cut off point were subjected to clinical examinations and measurement of serum TSH and T4 (thyroxin) levels by radioimmunoassay (TSH, IRMA; and T4 Kits, Immunotech Co., English). Neonates with primary diagnosis of hypothyroidism (T4 < 6.5 µg/dL and TSH > 10 mU/L) were taking levothyroxin and were monitored based on age. The data were analyzed using SPSS 11.5. The differences of serum TSH and T4 levels were evaluated by analysis of variance (ANOVA), followed by post hoc testing with Tukey′s test. The serum TSH levels were compared with categorical variables by the χ2 test. P < 0.05 was considered to be significant for statistical tests. Results The number of screened neonates, the recall rate, and the incidence of hypothyroidism are shown in [Table - 1]. The recall rate confirmed inadequate iodine intake in the area on the basis of the proposal made by WHO/UNICEF/ICCIDD. The frequency and number of neonates with blood TSH above the cut off point (5 mU/L) are shown in [Figure - 1]. [Figure - 2] shows serum TSH and T4 levels among neonates with blood TSH above the cut off point. There was significant association between the serum TSH and the blood TSH (subdivided into three ranges) as evaluated by ANOVA (P < 0.001). Also, we observed reverse association between serum T4 and blood TSH (P = 0.01). We found no significant correlation between serum TSH and sex (P = 0.62) and also between T4 levels and sex (P = 0.7). The female/male ratio was 1.4:1. Furthermore, there were no significant differences in the serum TSH and T4 levels between urban and rural regions (P = 0.33 and P = 0.47 respectively). Discussion In this study, we performed neonatal thyroid screening and evaluated the incidence of hypothyroidism in the eastern region of Iran. The screening was more practical in large areas because of the simple sampling procedure in this study as compared with that in some studies performed in Iran. [7] The data showed that the recall rate is high as compared with that in some countries of the region, such as Indonesia and Thailand. [8],[9] In some European countries, the recall rate was between 0.16% and 2.7%. [10],[11] Also, a recall rate of 1.6% with a cut off point of 20 µU/mL has been reported in Turkey. [12] Several studies have confirmed the validity of this policy as an acceptable index for evaluating iodine intake in populations. [13],[14] The frequency of neonatal blood TSH, spotted on filter paper, was above 3%, which indicated a mild iodine deficiency (ID) in the area on the basis of the proposal made by WHO/UNICEF/ICCIDD. Our results were in agreement with previous studies in Iran and the countries of the region. [15] The incidence of hypothyroidism was 2/1000, which is high as compared with that in other countries such as Finland, Hungary, and Turkey. [12],[16] Our patients were under treatment, and we could not distinguish between the forms of hypothyroidism. Since salt iodization program has reduced goiter rate in Iran, [17] we thought the transient type is the main form of hypothyroidism in the area. However, other factors such as antithyroid drugs, antithyroid agents produced in the body of the mother, and iodinated antiseptics might be involved in the incidence of hypothyroidism. In conclusion, we found high prevalence of hypothyroidism in the area. Furthermore, the frequency of blood TSH spotted on filter paper above cut off point indicated mild iodine deficiency in the area. The most important characteristics of screening performed as a focal point program were simple sampling and feasible transport of samples to the central laboratory. The procedure is practical for undeveloped and developing areas. We suggest a comprehensive policy should be developed in order to identify neonates with hypothyroidism and to monitor treatment in the studied population and neighboring countries, including Afghanistan, Pakistan, and Turkmenistan. References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08019f1.jpg] [ms08019f2.jpg] |
| |||||||||

{kind=link}
{kind=link}