 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
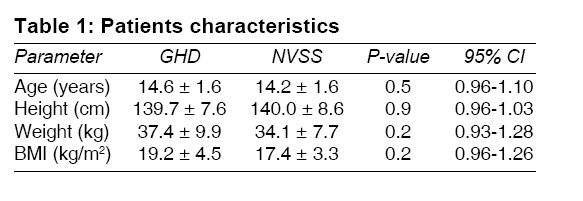
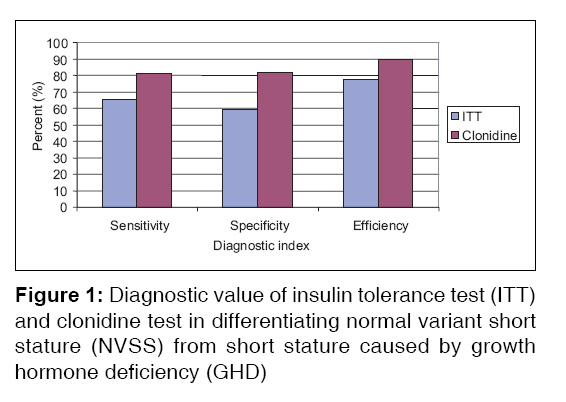
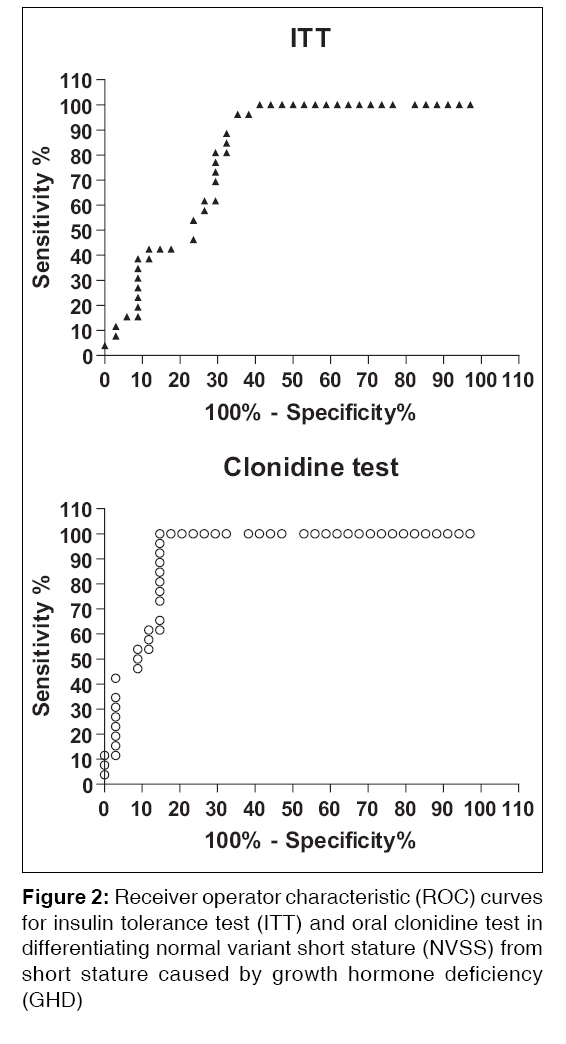
Indian Journal of Medical Sciences, Vol. 62, No. 4, April, 2008, pp. 149-156 ORIGINAL CONTRIBUTION Growth hormone deficiency short stature in a third world adult endocrine clinic: Usefulness of clonidine test in its diagnosis Al-Ruhaily AtallahD, Malabu UsmanH Department of Medicine (38), King Khalid University Hospital, Riyadh Code Number: ms08027 Abstract Background: Short stature (SS) can be treatable; yet the diagnostic value of a simple test in correctly identifying the two common etiologies in developing countries, viz., growth hormone deficiency (GHD) and normal variant short stature (NVSS), has not been reported in a typical third world population.Objectives: The aim of the study was to evaluate the reliability of clonidine test in differentiating short stature caused by GHD from NVSS. Settings and Design: Data of subjects evaluated for growth hormone deficiency SS at a Saudi Arabian university hospital were retrospectively reviewed. Materials and Methods: Clonidine and insulin tolerance tests (ITT) were conducted on 60 subjects aged 12 years and above with SS, while peak stimulated growth hormone cut off value of <10 µg/l was used to diagnose GHD. Statistical Analysis: Sensitivity and specificity for clonidine test and ITT were computed, while receiver operator characteristic (ROC) curves were constructed from the results in order to assess the diagnostic usefulness of the two tests. Mann-Whitney test was used to determine level of significance. RESULTS: Clonidine test showed superior sensitivity and specificity, viz., 81% and 82%, as against 65% and 59% for ITT respectively. Overall, the efficiency of clonidine test in correctly differentiating short stature caused by GHD from NVSS was higher, viz., 90%, compared to ITT's 77%. Conclusions: Clonidine test proved to be an excellent test for initial assessment of GHD and may be used as a screening test for short stature in third world countries. Keywords: Clonidine test, diagnostic usefulness, growth hormone deficiency, short stature, third world Introduction Short stature (SS) is common worldwide, and its clinical and psychosocial consequences are well known. For instance, in developing countries where health care facilities are limited, SS accounts for up to 16% of perinatal mortality. [1] On the other hand, in a Caucasian series, high suicide rate among subjects with short stature attributable to depression was recorded. [2] Early and prompt diagnosis is crucial to prevention of such devastating complications, for determining treatable causes of SS such as hypothyroidism and growth hormone deficiency (GHD). A number of diagnostic modalities have been sought in assessment of subjects with SS suspected to have GHD. These include simple and physiological tests such as exercise or sleep, but the performance characteristics of the tests have yet to be fully defined, resulting in low diagnostic efficiency. [3] Use of glucagon or arginine as growth hormone-stimulating test in detecting GHD is cheap but has to be administered parenterally, the latter in the form of infusion requiring close monitoring of side effects, with high false-positive results. [4] Concentration of serum insulin-like growth factor in short stature is reported to have high diagnostic efficiency for GHD, but its poor specificity in certain conditions causing short stature, such as malnutrition, limits its usefulness in developing countries. [5] Use of growth hormone-releasing hormone as provocative test in diagnosis of GHD is comparable to, or higher than, standard growth hormone stimulatory tests, but its high cost is a real limiting factor in its routine use in most centers. [6] Intravenous insulin administration by inducing hypoglycemia is a traditional gold standard criterion for diagnosis of GHD, [7] yet its reliability and safety in routine workup of SS have been challenged in recent reports. [4],[8] Orally administered clonidine, an alpha-2-adrenergic agonist, stimulates growth hormone release in normal subjects and was reported to play a useful diagnostic role in detecting SS caused by GHD in a number of studies. [9],[10] This laboratory parameter is simple and could be routinely performed in developing countries where SS and its complications are increasingly being encountered. [11],[12] However, the diagnostic value of clonidine test in correctly differentiating SS caused by GHD from NVSS has not been evaluated in a typical third world population. The present study was therefore undertaken to (i) evaluate the reliability of clonidine test in differentiating NVSS from short stature caused by GHD and (ii) to compare its diagnostic value with insulin tolerance test.Materials and Methods We conducted a retrospective investigation of patients who presented with, or were referred with, short stature to the adult endocrine clinic and were admitted for evaluation at King Khalid University Hospital (KKUH), Riyadh, Saudi Arabia, between 1 st January 2000 and 31 st December 2006. All hospital admissions were recorded electronically by the same medical record staff using codes according to the international classification of diseases (ICD). Data of patients with short stature and who were proven biochemically to have GHD and NVSS and admitted to the hospital during the 7-year period were retrieved from the records. Subjects aged 12 and above with height more than 3 SD below the mean for their age and sex on modified Tanner chart specific for the local population [13] and who satisfied the inclusion criteria highlighted below were evaluated for diagnostic value of ITT and clonidine test. Those with etiologies of SS other than GHD and NVSS were excluded from the study. For each patient, the following information was recorded: chronological age, family history of SS, birth asphyxia, birth weight (if available), attainment of developmental milestones, and longstanding diarrhea or abdominal pains, as well as usage of medications known to cause short stature. All positive clinical findings detected during general and systemic examination, including anthropometric measurements, were recorded. Informed consents from patients and/or relatives were acquired, while approval for laboratory and clinical review was obtained from the ethics committee of KKUH. Laboratory investigations performed included complete blood count, urine examination, and biochemical tests including serum concentrations of glucose, urea, creatinine, sodium, potassium, calcium, phosphorus, alkaline phosphatase, total proteins, and albumin. An X-ray of the left wrist was taken in every patient, while additional X-rays (elbow, knee, and hip-pelvis) were taken in older children to determine approximate bone age assessed according to the atlas of Greulich-Waterhouse and Pyle. [14] To characterize the etiology of hypopituitarism, MRI pituitary was done in patients with GHD. To assess for Turner′s syndrome, cytogenetic studies were conducted on every female subject. Serum IgA endomyesial antibody was determined for all patients; and upper gastrointestinal endoscopy and biopsy were done for those who proved positive, in order to exclude celiac disease. Renal tubular acidosis was excluded in subjects with clinical and radiological evidence of rickets by conducting urinary acidification test according to standard protocol. Diabetes insipidus was assessed and excluded in patients with 24-hour urinary volume of greater than 50 ml/kg body weight by subjecting them to dehydration test. [15] GH stimulation was achieved with two dynamic tests after 12- to 14-h overnight fasting, first day ITT, followed by clonidine test the next day. The clonidine test was conducted as described by Gil-Ad et al.[10] using an oral dose of 0.15 mg/m 2 body surface area. The drug was given as Catapres tablets, each of which contains 150 ug and the dose was rounded off to the nearest 75 ug half tablet. Blood samples for GH levels were taken from an indwelling catheter at 0, 30, 60, 90, 120 min after medication. Blood pressure was measured half hourly throughout the procedure, and patients were observed in the ward for a further hour before going home. The ITT was carried out using human regular insulin (Humulin) in an intravenous dose of 0.15 U/kg body weight after an overnight fast. As in clonidine test, samples of the GH analysis were taken half hourly for 2 h through an indwelling intravenous cannula, and all samples were also assayed for glucose and cortisol. In both tests, a maximum GH concentration of 10 µg/l or greater was taken to exclude GH deficiency. [8],[16] A peak GH response less than 10 µg/l was considered abnormal for both the tests. Side effects were monitored. Intravenous hydrocortisone and 50 ml 50% dextrose were reserved for use in case of severe symptoms of hypoglycemia. Hormonal analyses conducted included basal growth hormone (GH), cortisol, free triiodotyronine (FT3), free tetra-iodotyronine (FT4), thyroid stimulating hormone (TSH), and gonadotropins. All the GH tests were done in the morning after an overnight fast, and hormone estimation was performed by specific radioimmunoassay. GH, FT3, FT4, TSH, and luteinizing hormone estimates were performed by electrochemiluminescence immunoassay (Roche Diagnostics, Indianapolis, IN, USA) with intra-assay and inter-assay coefficient of variation less than 2% and less than 5%, respectively. Growth hormone deficiency (GHD) was defined as peak stimulated serum growth hormone level of < 10 µg/l documented by both tests. [8] NVSS was diagnosed when stimulated serum growth hormone level of 10 µg/l or greater was recorded in at least one test in the absence of any other identifiable cause of SS. [16] Estimates of sensitivity [true-positive results/(true-positive results + false-negative results)], specificity [true-negative results/(true-negative results + false-positive results)], and diagnostic accuracy were determined for both ITT and clonidine test in differentiating short stature caused by GHD from NVSS. To further characterize the diagnostic usefulness of the two tests in discriminating the two diagnoses, we constructed univariate receiver operating characteristic curves (ROCs) by plotting the sensitivity against (1 − specificity) using dedicated software. The results are given as mean ± standard deviation. For statistical analysis, Mann-Whitney test was used. A P-value < 0.05 was considered significant. Results In all, 60 subjects (38 males and 22 females; age range, 12-21 years) with SS were assessed for diagnostic usefulness of ITT and clonidine test. Twenty-six subjects were proved to have GHD, while 34 had NVSS. Mean age and anthropometric measurements in the two groups of subjects who had hypoglycemic and clonidine tests were similar, as shown in [Table - 1]. GHD was excluded in 34 subjects, whose responses to either of the tests were normal and thus were diagnosed as NVSS with peak GH response to hypoglycemia being 15.8 ± 13.5 µg/l; and to clonidine, 15.8 ± 8.6 µg/l, P > 0.05. On the other hand, mean peak GH response to hypoglycemia and clonidine in subjects diagnosed as GHD was 5.1 ± 2.2 µg/l and 5.2 ± 2.4 µg/l respectively, P > 0.05. Adequate hypoglycemia and cortisol responses were achieved in all subjects undergoing ITT, while blood pressure was closely monitored during the clonidine test. Side effects of the two procedures were looked for. None of the subjects evaluated developed severe symptoms from the two tests. However, all the 60 subjects (100%) on ITT and 21 (35%) who received clonidine complained of drowsiness. Thirty-nine (65%) of the subjects on clonidine test had hypotension, while 1 patient on ITT experienced nausea. All the symptoms resolved following oral feeding upon completing the tests, without any of them being persistent. Of the 60 pairs of tests, the results agreed in 40 pairs (66.7%). Of the remaining 20 pairs with discordance, six patients had a normal response to insulin only and 14 had a normal response to clonidine only. The distribution of hormonal profile in patients with SS revealed, unlike ITT, clonidine test achieved near-perfect discrimination between NVSS and GHD. Using cut off values of < 10 µg/ml, clonidine test correctly diagnosed GHD in patients with SS, viz., 90%, as compared to 77% for ITT, as depicted in [Figure - 1]. Analysis of the ROC curve of the ITT and clonidine test is shown in [Figure - 2]. With respect to the standard criterion of maximally attained GH response to each test, the sensitivity and specificity were 81% and 82% for clonidine test, compared to 65% and 59% for ITT, respectively as presented in [Figure - 1]. The ROC curve plots the true-positive rate (sensitivity) against the false-positive rate (1 − specificity) for the cut-point of GH 10 µg/l. A test with perfect discrimination between GHD patients and NVSS subjects (100% sensitivity and 100% specificity) would coincide with the left upper corner of the graph and be associated with ROC area of 1.0. In contrast, a test providing no discrimination between the two groups would result in a diagonal line from the left lower to the right upper corner of the panel (sensitivity = 1 − specificity) and correspond to ROC area of 0.5. Discussion We have shown that clonidine test offers excellent discrimination in the diagnosis of short stature caused by GHD vis-a-vis that caused by NVSS. Of the two diagnostic parameters tested, clonidine test showed higher overall diagnostic efficiency. It demonstrated best combination of results for sensitivity and specificity in identifying GHD in subjects presenting with short stature. The potential value of using clonidine test is of particular interest, as this method has not been preferentially used previously in third world countries where modern diagnostic facilities are scarce and, when available, often beyond the reach of an average parent or patient. Indeed, the test correctly identified 28 of the 34 subjects with SS caused by NVSS, which was similar to others′ findings. [9],[10] Identification of GHD in SS using simple and readily available tools may prove to be a misleading concept. For instance, nonpharmacological exercise test, though easy to perform, is reported to have as low as 11% specificity compared to standard growth hormone-provocative tests. [3] Similarly, ITT has been found to be poorly reproducible in normal and GHD subjects and is associated with wide coefficient of variation, thus questioning its diagnostic efficiency as preferred initial test of choice in the assessment of SS. [4],[8] Moreover, ITT is contraindicated in patients with ischemic heart disease, seizure disorders, and extreme ages. [4],[17] On the other hand, clonidine test has been proved to have better diagnostic usefulness and safety profile than ITT, and the former may be used as a screening test for subjects with SS. [9],[10],[18] Hypotension and drowsiness were the common side effects of clonidine test reported, occurring in up to 80% of subjects in earlier series, as well as in our current report. [10],[19] Interestingly, despite the relatively high incidence of adverse effects of clonidine, none of our patients had severe symptoms requiring resuscitative intravenous fluid administration during the procedure, which was similar to observations made earlier by others. [18],[19] It is important to address the validity of our conclusions. We tested the diagnostic value of two growth hormone-provocative tests in SS subjects for diagnosis of GHD and NVSS after exclusion of other etiologies of the condition in a retrospective data derived over a 7-year period. Diagnoses were based on growth hormone responses following two stimulatory tests, namely, ITT and clonidine test, in line with recent recommendation for diagnosis of GHD. [8],[16] Although use of more than two stimulation tests in our cohort may affect the diagnostic indices, we believe the overall pattern of comparison between the two tests is not likely to be affected if other pharmacological tests were to be added, as demonstrated by Biller et al. in a recent analysis of six stimulatory tests for GHD. [20] In addition, serum IGF-1 and IGFBP-3 levels were not determined in this study as both have been proved to have low sensitivity and inferior diagnostic efficiency in malnutrition-prevalent third world population. [21] Furthermore, it is important to acknowledge the shortcomings associated with retrospective studies in general. Observations derived from such studies may contain some missing information and thus may serve as a stimulus to further prospective work to clarify findings. The present work must be interpreted keeping in mind the defects inherent in such studies. Despite these limitations, our results are in agreement with observations made earlier by others. [9],[10],[18] Indeed, receiver operator characteristic clearly demonstrated higher diagnostic usefulness of clonidine test compared to ITT in correctly identifying SS subjects with GHD. In conclusion, this study demonstrated superior diagnostic accuracy of clonidine test compared to ITT as a procedure of choice in the initial assessment of subjects with SS. In terms of simplicity and cost-effectiveness, use of clonidine test may have considerable advantage over ITT in investigating SS suspected to have GHD. Further studies on a larger population are however needed to verify our findings. Acknowledgment We are grateful to Dr. Monsur Kazi for his advice regarding statistics; and Mirza Ahmed and Fahad Al-Otaibi for deciphering ROC curves and secretarial assistance respectively.References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08027f1.jpg] [ms08027t1.jpg] [ms08027f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}