 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
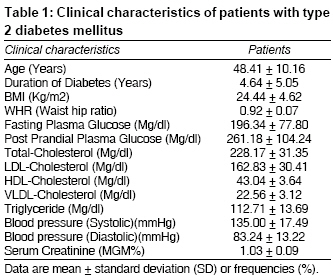
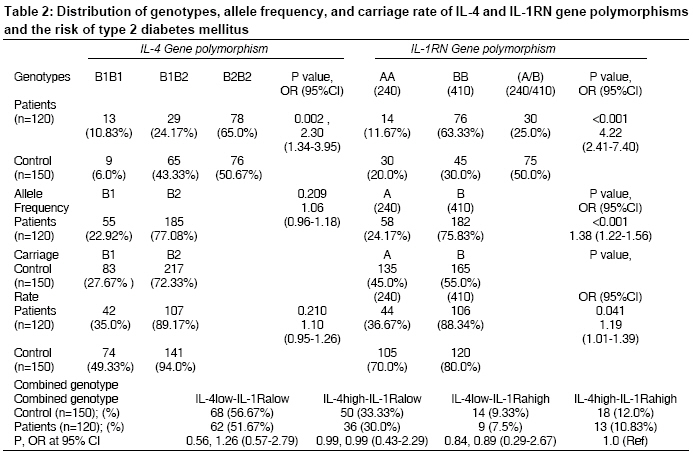
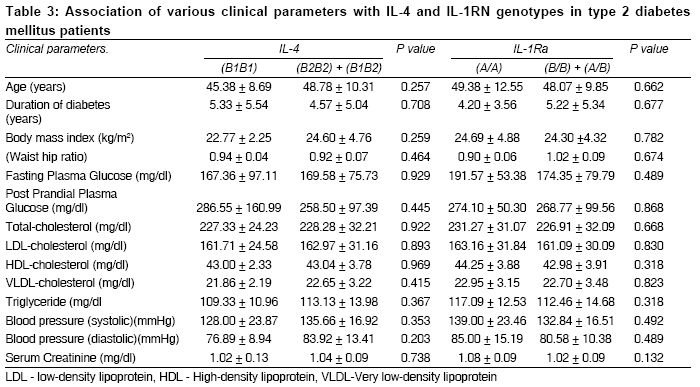
Indian Journal of Medical Sciences, Vol. 62, No. 7, July, 2008, pp. 259-266 ORIGINAL CONTRIBUTION Association of IL-4 and IL-1RN (receptor antagonist) gene variants and the risk of type 2 diabetes mellitus: A study in the north Indian population Bid HemantKumar, Konwar Rituraj, Agrawal CG, Banerjee Monisha Department of Zoology, University of Lucknow, Lucknow Code Number: ms08047 Abstract Background: Inflammation is a key event closely associated with the pathophysiology of type 2 diabetes mellitus (T2DM). Association of genetic polymorphisms of inflammatory cytokines with T2DM is largely unknown. Our objective was to investigate the relationship of polymorphism of IL-1RN and IL-4, two important biomarkers of inflammation, with the risk of T2DM. Keywords: IL-4, IL-1RN, polymorphism, type 2 diabetes mellitus Introduction Type 2 diabetes mellitus (T2DM) is manifested by hyperglycemia resulted from resistance to insulin in fat, muscle, and other key target tissues of insulin; and decreased insulin secretion by beta cells of islets of Langerhans. Chronic low-grade inflammation and activation of the innate immune system are closely involved in the pathogenesis of T2DM. [1] Recently, T2DM has also been recognized as an immune-mediated disease leading to impaired insulin signaling and selective destruction of insulin producing beta-cells in which cytokines play an important role. [2],[3],[4] Cross-sectional studies have provided support for the hypothesis that chronic subclinical inflammation may be associated with insulin resistance and may precede the development of clinically overt T2DM. [5] IL-4 is an important anti-inflammatory cytokine that directs macrophages towards a phenotype that is characterized by the elaboration of other anti-inflammatory molecules, like IL-10, IL-1RN, and IL-1R2. IL-4 shifts the inflammatory balance by inhibiting the secretion of the pro-inflammatory cytokines IL-1beta, TNF-alpha, and IL-6 from macrophages. Disturbance of the anti-inflammatory response could be a critical component of the chronic inflammation found in T2DM. Type 2 diabetes mellitus disrupts anti-inflammatory cytokine function of IL-4 as a mediator of production of antagonist of interleukin-1 (IL-1RN). [6] IL-1RN, a naturally occurring competitive inhibitor of IL-1, binds to the type I receptor and protects human pancreatic cells from IL-1beta-induced functional impairment and apoptosis. [7],[8] Claus et al. proposed that IL-1RN has possible therapeutic potential in the treatment of T2DM. [9] Recently, it was indeed revealed that administration of IL-1RN in the form of Anakinra has been successfully shown to improve beta cell function in patients with T2DM. [10] The nature of association of IL-4 and IL-1RN polymorphisms with, and their combined effect on, Indian T2DM patients is not known. As a first step to evaluate whether these cytokines′ polymorphisms have functional influence on the susceptibility to T2DM, we conducted a study of the association of the gene polymorphisms of IL-4 and IL-1RN with diabetes in a population-based study in the Indian population. Materials and Methods Patients and clinical evaluation Screening and management of patients was done as per American Diabetes Association guidelines. [11] Subjects were included in the diabetes group if they had fasting glucose concentrations ≥126 mg/dL or 2-hour glucose concentrations ≥200 mg/dL after a 75-g oral glucose tolerance test with all clinical details. [12] A total of 120 subjects after screening were included in this study. A questionnaire was used to record clinical history of diabetes and associated complications, hypertension; as well as family history. After screening with standard oral glucose tolerance test, a total of 150 age- and BMI-matched normal healthy controls were enrolled from among the healthy staff members of the institute and university for this study. Subjects having history of coronary artery disease or other metabolic disorders were excluded from the control group. Sample processing and genotyping IL-4 intron-3 VNTR IL-1RN exon-2 VNTR The molecular weight of each band was determined by using the software in Biovis Gel Software, version 4 (Expert Vision, Mumbai), and the unknown samples were compared with the 100 bp DNA ladder (MBI-Fermentas, USA). To improve the genotyping quality and validation, 20% of samples were re-genotyped by other laboratory personnel, and the results were found to be reproducible with no discrepancy noticed in genotyping. Genotyping of 10% of samples was confirmed by DNA sequencing Statistical analysis Results A total of 120 T2DM patients (mean age, 48.41 ± 10.16 years) and 150 healthy controls (mean age, 50 ± 11.28 years) were evaluated for the IL-1RN and IL-4 gene polymorphism study. The mean blood pressure, plasma glucose, cholesterol (LDL/HDL/VLDL/total), serum creatinine, and other parameters are listed in [Table - 1]. The comparative distribution of genotype in patients versus controls showed that overall genotype distribution for both IL-4 ( P = 0.002) and IL-1RN ( P < 0.001) gene polymorphisms was significantly associated with T2DM patients [Table - 2]. In regard to allele frequency and carriage rate, there was lack of association in case of IL-4 ( P = 0.209 and .210 respectively) among patients and controls. However, a significant difference in both allele frequency and carriage rate ( P < 0.001 and P = 0.041 respectively) was observed for IL-1RN gene polymorphism [Table - 2]. The genotype frequency of BB (63.3% vs. 30.0%) and allele frequency of B (75.83% vs. 55.0%) of IL-1RN were significantly higher in patients than in controls. Similarly, in case of IL-4 the frequency of B2B2 genotype (65.0% vs. 50.67%) and that of B2 allele (77.08% vs. 72.33.0%) were significantly higher in patients than in controls [Table - 2]. In order to investigate gene-gene interaction, we analyzed the combined effect of IL-4 and IL-1RN on, and their possible association with, T2DM . Genotypes were grouped into high- or low-producer phenotypes - IL-4, B1B1, or B1B2 = high-producer (HP) phenotypes; B2B2 = low-producer (LP) phenotypes. Similarly in case of IL-1RN, AA = HP phenotypes, and all others were considered LP phenotypes. Comparative analysis of combinations of IL-4 and IL-1RN (IL-4 low -IL-1RN low / IL-4 high -IL-1RN low / IL-4 low -IL-1RN high ) showed that all these combinations lacked significant difference ( P = 0.56, 0.99, and 0.84 respectively) between controls and T2DM patients [Table - 2]. IL-4 and IL-1RN high-producing genotypes were taken as reference for this analysis. We also analyzed the association of different clinical parameters of T2DM patients with IL-4 and IL-1RN genotypes; there was lack of association with any of these parameters [Table - 3]. Discussion Earlier studies have reported that hyperglycemia associated with T2DM acutely increases peripheral cytokines like IL-6 and TNF-α and IL-1 proteins. [16] In vitro studies revealed that IL-6 and TNF-alpha can impair insulin-signaling pathway, resulting in insulin resistance. [17],[18] It is proposed that cytokines might normally function in a feedback pathway to limit the number of adipocytes or lipid storage by exerting catabolic effects on the adipocyte, blocking lipid synthesis and lipoprotein lipase expression, while activating lipolysis, and can block or reverse differentiation of fibroblastic precursors into adipocytes. [19] However, in vivo results till date are largely inconsistent. Identification of appropriate markers of T2DM for recognizing genetic influence upon initiation and progression of the disease might assist the clinicians in adopting a more precise approach for the identification of ′high-risk′ T2DM patients and in the development of personal medicine strategies for targeting inflammatory components; thus meeting a crucial medical need, as well as enabling planning therapeutic interventions. Genetic polymorphisms studied so far in T2DM with TNF-α and IL-6 have also revealed no or only marginal association. [20],[21] Lisa et al. reported lack of association of IL-4 with type 1 diabetes mellitus, but the nature of association of IL-4 with T2DM is unknown. [22] Recently, Achut et al. demonstrated a significant association of VNTR polymorphism of IL-4 with increased risk of T2DM, as well as its associated complications in the north Indian population. [23] In our study, we have also found positive association of not only IL-4 but also of IL-1RN genotype with T2DM. It is already shown that T2DM inhibits IL-4-mediated IL-1RN production, and administration of IL-1RN improves T2DM. Thus our current findings suggest that genetic polymorphism of both IL-4 and IL-RN may finally influence initiation and progression of T2DM as already reported. Measurement of the IL-4 and IL-1RN levels in serum, along with the association studies of polymorphism, would further strengthen the predicted functional implications; however, this was one important limitation of this study. Besides, like many other significantly associated cytokine polymorphisms in T2DM, how these cytokines induce insulin resistance and help in progression of the vicious cycle of insulin resistance and beta cell degradation is largely unknown. Since both IL-1RN and IL-4 have been found to be associated with risk of T2DM, it was imperative to investigate if combination of their particular polymorphic variants could specifically influence the susceptibility further. Therefore, we also tried to find out the combined effect of IL-1RN and IL-4 on T2DM and observed that IL-4 low -IL-1RN low genotype showed 1.26 times risk compared to IL-4 low -IL-1RN high and IL-4 high -IL-1RN low in patients, although the P value was not significant. In conclusion, this study supports that genetic variation in IL-4 and IL-1RN cytokine genes may predispose to the development of T2DM in the Indian population. The combined effect of IL-4 and IL-1RN revealed a further increase in risk of T2DM. Acknowledgment Department of Biotechnology, Govt. of India, for funding the work.References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08047t1.jpg] [ms08047t3.jpg] [ms08047t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}