 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
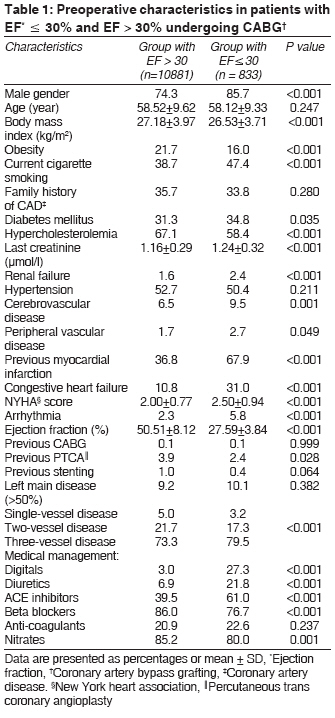
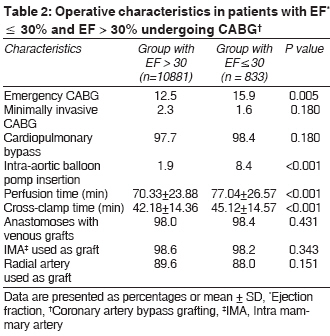
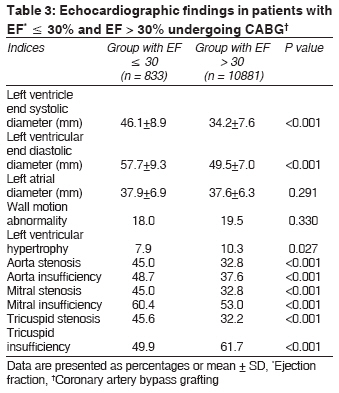
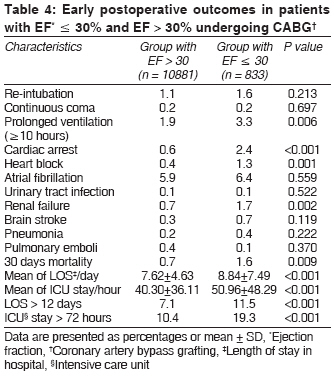
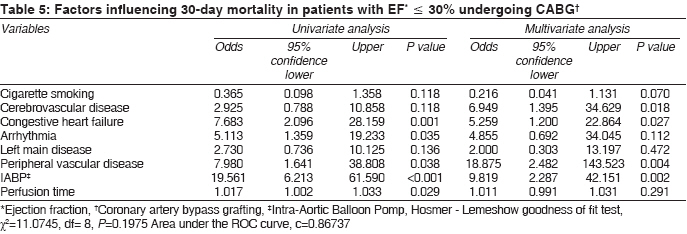
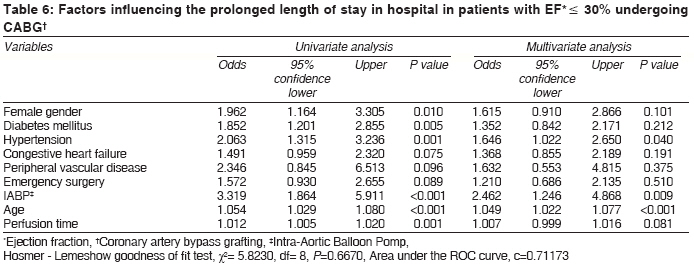
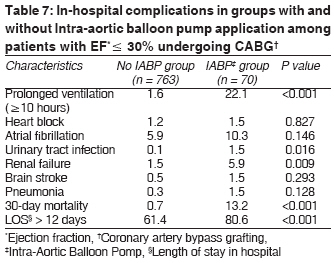
Indian Journal of Medical Sciences, Vol. 62, No. 8, August, 2008, pp. 314-322 ORIGINAL CONTRIBUTION Coronary artery bypass grafting in patients with low ejection fraction: The effect of intra-aortic balloon pump insertion on early outcome Davoodi Saeed, Karimi Abbasali, Ahmadi Seyed Hossein, Marzban Mehrab, Movahhedi Namvar, Abbasi Kyomars, Omran Abbas Salehi, Shirzad Mahmood, Sheikhvatan Mehrdad, Abbasi Seyed Hesameddin Department of Cardiac Surgery, Tehran Heart Center, Tehran University of Medical Sciences, Tehran Code Number: ms08057 Abstract Background: Survival benefit with intra-aortic balloon pump (IABP) insertion for coronary artery bypass grafting (CABG) patients with left ventricular dysfunction is controversial. The aim of this study was to assess the early results of CABG that predict 30-day mortality and prolonged length of hospital stay (LOS) after isolated CABG and the role of IABP application as a main predictor in patients with an ejection fraction (EF) of 30% or less. Keywords: Coronary artery bypass grafting, intra-aortic balloon pump, left ventricular dysfunction, outcome Introduction Some randomized controlled trials showed a survival benefit with intra-aortic balloon pump (IABP) insertion for coronary artery bypass grafting (CABG) patients with low ejection fraction (EF). [1],[2] Also, it has been clear that IABP is an effective means of supporting failing circulation in patients at high risk of cardiovascular events post-operatively. [3] However, IABP is an intensive care-based treatment and is therefore costly. In addition, it can be accompanied by complications including limb ischemia, aortic or iliac dissection bleeding, infection, hemolysis, paraplegia, and stroke. [4],[5] Any survival benefit after CABG in the face of severely depressed LV function is relatively known; however, determination of factors such as IABP, which affect this survival, is necessary. Furthermore, there has been no widespread recognition of the results of IABP procedure in these patients. We aimed to develop multivariable models of preoperative, operative, and postoperative risk factors that predict 30–day mortality and prolonged length of stay (LOS) in hospital after isolated CABG and also determine the effect of IABP support on these outcomes in patients with an ejection fraction of 30% or less. Materials and Methods Demographic and clinical characteristics of 11714 patients undergoing isolated CABG (833 patients with LVEF ≤ 30% as the study group and 10881 patients with EF > 30% as the control group) from 1 January 2002 to 1 January 2007 were collected and entered into a computerized database. All patients with the history of concomitant cardiac and non-cardiac operations were excluded. Final determination of ejection fraction was based on angiographic reports. In this study, CAD was considered significant if there was a 75% or greater stenosis in the cross-sectional diameter and 50% or greater stenosis in the luminal view. [6] The following variables were collected for statistical analysis including the preoperative variables: 1) general characteristics: age, gender, and body mass index; 2) preoperative risk factors (total cholesterol ≥ 5.0 mmol/l, HDL-cholesterol ≤ 1.0 mmol/l in men, or ≤ 1.1 mmol/l in women, triglyceride ≥ 2.0 mmol/l), [8] (first-degree relatives before the age of 55 in men and 65 years in women), [9] (systolic blood pressure ≥ 140 mmHg and/or diastolic ≥ 90 mmHg and/or on anti-hypertensive treatment), [10] n ≥ 11.1 mmol/l or fasting plasma glucose ≥ 7.0 mmol/l or 2–hp ≥ 11.1 mmol/l renal failure (creatinine > 355 µmol/l with a rise of > 44 units or urine output below 0.3 ml/kg for 24 h), cerebrovascular disease, peripheral vascular disease, and chronic lung disease; 3) preoperative cardiac status: recent myocardial infarction (an acute event with abnormal creatine phosphokinase and troponin levels), New York Heart Association (NYHA) score, arrhythmia, and previous CABG and PCI; and 4) preoperative homodynamic status: number of defective coronary vessels, left main disease ≥ 50%, and LVEF. The operative data included type of surgery (elective or emergency), the number of distal anastomoses with vein grafts, the use of internal mammary artery (IMA) as grafts, and the use of IABP. We considered four criteria for a complicated postoperative short-term outcome: 1) in-hospital postoperative complications including at least one of these: cardiac complications (heart block, cardiac arrest, tamponade, and atrial fibrillation) and non-cardiac complications (brain stroke, transient ischemic attack, renal failure, urinary tract infection, pulmonary emboli, pneumonia, acute limb ischemia, multi-system failure, continuous coma≥ 24 hours, and prolonged ventilation≥10 hours); 2) prolonged LOS in ICU before and after surgery; 3) prolonged hospital stay before and after operation; and 4) 30–day mortality rate (sometimes termed operative mortality) defined as death within 30 days of operation. [12] Results were reported as mean ± standard deviation (SD) for quantitative variables and percentages for categorical variables. The groups were compared using the student′s t-test for continuous variables and the chi-square test or Fisher′s exact test if required for categorical variables. The analysis of covariance (ANCOVA) was used as the multivariate analysis for the evaluation of differences in LOS between the study and the control groups in the presence of possible confounding factors. Predictors exhibiting a statistically significant relationship with 30–day mortality and prolonged LOS in the univariate analysis (P value equal or less than 0.15) were taken for a multivariate logistic regression analysis to investigate their independence. Odds ratios (OR) and 95% confidence intervals (CI) for OR were calculated. Model discrimination was measured using the c statistics, which is equal to the area under the ROC (Receiver Operating Characteristic) curve. Model calibration was estimated using the Hosmer-Lemeshow (HL) goodness-of-fit statistic (higher P values imply that the model fits the observed data better). The data analyzer was anonymous, and data collection and processing were approved by the institutional review board of our heart center. P values of 0.05 or less were considered statistically significant. All the statistical analyses were performed using SPSS version 13 (SPSS Inc., Chicago, IL, USA) and SAS version 9.1 for Windows (SAS Institute Inc., Cary, NC, USA). Results The two groups were similar with respect to mean age ( P = 0.247) [Table - 1]. There were no significant differences between the two groups in terms of family history of CAD and hypertension. Among the risk factors, hypercholesterolemia ( P < 0.001) and obesity ( P < 0.001) were more prevalent in the patients with EF > 30, whereas other risk factors were more frequent in the patients with severe left ventricular dysfunction. According to the medical management, within 24 hours preceding surgery, some drugs such as digitalis, diuretics, and ACE-inhibitors were administered more in low EF group prior to surgery, whereas nitrates and beta-blockers were used more in another group [Table - 1]. There was a significant difference in the number of defective vessels between the two groups, so that three-vessel disease was found more common in patients with severe left ventricular dysfunction ( P < 0.001). Both arterial and venous grafts were similar in the two groups [Table - 2]. Emergency CABG was more frequent in the patients with severe left ventricular dysfunction ( P = 0.005). Furthermore, IABP was significantly used more in patients with EF less than 30% ( P < 0.001). According to the echocardiographic findings, no significant differences were found in the left atrial and left ventricular diameters between the two groups; however, except for tricuspid valve insufficiency that was more frequent in the group with higher EF, other valvular pathological changes were found higher in the group with lower EF [Table - 3]. Rates of complete revascularization were similar between the group with lower EF and another group (84.4% vs . 85.7%, P = 0.342). Clinical outcomes and postoperative complications are detailed in [Table - 4]. Prolonged ventilation (>10 hours), cardiac arrest, heart block, and renal failure were more prevalent in the severe left ventricular dysfunction group; however, there were no statistically significant differences between the two groups in terms of other postoperative complications. The thirty-day mortality rate ( P = 0.009), length of stay in ICU ( P < 0.001) and in hospital, before and after surgery, ( P < 0.001) were also higher in the severe ventricular dysfunction group. Covariance analysis also showed that the LOS was longer in lower EF group ( P < 0.001). Furthermore, multivariate logistic regression analysis revealed that the early mortality rate was slightly higher in this group ( P = 0.075). Multivariate logistic regression analysis showed that in patients with severe left ventricular dysfunction, the use of IABP ( P = 0.002), congestive heart failure ( P = 0.027), peripheral vascular disease ( P = 0.004), and history of cerebrovascular disease ( P = 0.018) were related to the 30–day mortality rate [Table - 5]. In addition, prolonged length of stay in hospital in these patients was related to IABP ( P = 0.009), hypertension ( P = 0.040), and the increase of age ( P < 0.001) [Table - 6]. Early complications in patients with and without IABP application are summarized in [Table - 7]. All studied complications were numerically more common in IABP application group; however, urinary tract infection, prolonged ventilation, renal failure, mortality, and prolonged LOS were statistically more frequent in this group. Discussion The role of IABP application is well known as a death related risk factor in patients who undergo CABG. [13] However, mortality, morbidity, and long-term prognosis of patients with low LVEF who underwent concomitant CABG and IABP were not as optimistic as those of patients with normal cardiac function and the assessment of outcome of these patients in variant population is necessary. In our study, however, perioperative mortality was 1.6% in patients with EF ≤ 30%, which was significantly higher than that in patients with greater EF, and this mortality was strongly influenced by IABP application. Similarly, in a study by Aksnes et al. , insertion of IABP was a strong predictor of death for patients in need of IABP support in the course of cardiac surgery. [14] Arafa et al. found a mortality rate of 52.6% in patients undergoing cardiac operations who required the use of an IABP and confirmed that the early mortality rate in patients who received an IABP was high. [15] Although the beneficial effects of IABP treatment in high-risk patients who have coronary artery bypass grafting have been shown, [16],[17],[18] determination of the main factors that can influence the IABP-associated mortality in low EF patients is recommended. In the present study, prolonged LOS was observed even more in patients with IABP application. It can be related to the higher occurrence of postoperative in-hospital complications, which need to be managed and removed before discharge in this group. In the present study, no difference in 30–day mortality between the two genders was found. Similarly, in the Argenziano study, no relation was found between 30–day mortality and gender, [19] whereas in the Wang studies, the female gender was a main predictor of mortality. [14] Some of the suggested contributing factors in women are advanced age, advanced disease, comorbidities, and smaller body surface area. [20] Also, in both Argenziano [19] and our studies, advanced age was not a risk factor for mortality, but this relation was seen in other studies. [20],[21] In our study, congestive heart failure was a strong risk factor for 30–day mortality in patients with left ventricular dysfunction. In the Argenziano et al. study, mortality was significantly higher in patients with preoperative symptomatic heart failure. [19] Patients with severe congestive heart failure have been previously shown to have four times the mortality rate after bypass compared to patients with better ventricular performance. [22] Improvements in the ejection fraction may have a beneficial effect on survival, and this is likely to be greatest in patients with severe left ventricular dysfunction. [23],[24] In our study, female gender was an important predictor for prolonged length of stay in hospital and this result was also found in the Borzak study. [25] In several studies, female sex is reported to be an independent predictor of length of stay in hospital. [26],[27],[28] It seems that the most common causes of prolonged length of stay in hospital in females are higher incidence of preoperative risk factors and postoperative complications of CABG in female than male. [29] Therefore, it is important to control these risk factors in female patients before operation. In the present study, only 8.4% of patients in the low ejection fraction group were on IABP. We believed that the surgeons have different indications about IABP insertion and it seems that the use of IABP is dependent on the surgeons′ perception. Also, because of the shorter perfusion time and cross-clamp time in our research in comparison with other previous reports in Iran [30] and other countries, [31],[32],[33] our data about the frequency of IABP insertion could be lower than the other reports. Conclusion Low ejection fraction can positively affect thirty-day mortality and prolonged LOS and ICU stay in patients who undergo CABG. One of the most important predictors of the 30–day mortality rate and prolonged LOS was IABP insertion. Furthermore, IABP application can increase early postoperative complications. Although left ventricular dysfunction is itself an important risk factor in patients undergoing CABG, the early outcome of CABG in patients with left ventricular dysfunction is acceptable and the management of this factor will help to reduce the mortality and total length of stay in hospital. Acknowledgment This research project has been supported by Medical Sciences/University of Tehran. We are indebted to Dr. Shahin Akhoundzadeh and Dr. Soheil Saadat, for technical assistance and Dr. Mahmoud Sheikhfatollahi for statistical analysis. The authors would like to thank the interviewers who collected the information and the participants who gave up their time for the study.References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08057t5.jpg] [ms08057t7.jpg] [ms08057t4.jpg] [ms08057t1.jpg] [ms08057t2.jpg] [ms08057t6.jpg] [ms08057t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}